ADDIN CNKISM.UserStyleStandards and problems for epidemic prevention in buildings: a review
*Correspondence to:
Lei Yuan, Lab for Optimizing Design of Built Environment, School of Architecture and Urban Planning, Shenzhen University, Shenzhen 518060, Guangdong, China.
E-mail: yuanlei@szu.edu.cn
J Build Des Environ. 2023;1:6202. 10.37155/2811-0730-0101-4
Received: June 18, 2022Accepted: September 01, 2022Published: November 10, 2022
Abstract
The complexity of the building environment directly affects the spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) inside the building. Therefore, the paper systematically reviewed the effective and feasible measures, designs and relevant epidemic prevention guidelines formed in the field of epidemic prevention during the period of COVID-19, as well as the excellent research and projects around the world. The study found that most of the people infected with COVID-19 were infected indoors, but the current building design was not included in the scope of epidemic prevention design, not effectively resist the spread of infectious diseases, and there is no standard guideline for epidemic prevention building design so far. Therefore, it is necessary to formulate building epidemic prevention standards, and by considering the epidemic prevention design in the architectural planning and design stage, the use of building epidemic prevention products, healthy wind environment design, etc. to establish a healthy building environment can effectively reduce the risk of epidemic transmission inside the building. However, due to insufficient epidemiological data and pathological research on the risk of epidemic transmission among residents, further research on the standards for epidemic prevention and quantitative risk assessment methods of building is limited.
Keywords
SARS-CoV-2, COVID-19, epidemic prevention, building, epidemic normalization
1. Introduction
COVID-19 caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) broke out in December 2019 and was declared a pandemic virus by the World Health Organization on March 11th, 2020[1]. With the arrival of the normalization stage of epidemic prevention, major changes have taken place in human production and lifestyle[2]. In particular, reported cases associated with buildings, including residential buildings, commercial buildings, schools, hospitals, airports, ports, cold chain logistics and other buildings, infected with the new coronavirus are common, attracted great attention from all walks of life.
Buildings are gradually becoming the source of epidemic infection with the greatest risk, such as COVID-19, and therefore an important battlefield for epidemic prevention[3]. However, at present, the government and medical personnel are the main forces formulating anti-epidemic systems and implementing anti-epidemic measures, and most of the epidemic is transmitted in closed places such as offices, meeting rooms, vehicles and schools[4]. Moreover, according to national standards (Table 1), the current architectural design mainly stipulates the static concentration index of pollutants, but does not consider using natural or other design means to reduce the concentration and transmission path of pollutants in architectural design.
| Name | Nation | Contents related to epidemic prevention |
| Assessment standard for healthy building | China | Ventilation, air conditioning, entrance, sunshine |
| Guidelines for epidemic prevention design and safety guarantee of indoor air environment in public and residential buildings (Trial) | Ventilation, air conditioning, window spacing, floor spacing, fresh air volume, water treatment | |
| Guidelines for emergency operation and management of office buildings for dealing with “novel coronavirus” T/ASC 08-2020 | Ventilation and air conditioning,Water supply and drainage system,System cleaning and cleaning disinfection,Garbage collection and temporary storage | |
| Technical guide for epidemic prevention and control in shopping malls and supermarkets | Wear masks, ventilation, cleaning and disinfection, cold chain food requirements, current and distance limiting measures | |
| WELL series | the United States | Ventilation, disinfection, air and water quality monitoring |
| WELL Health-Safety Rating | Cleaning and Sanitization Procedures,Emergency Preparedness Programs,Air and Water Quality Management | |
| ASHRAE Standards and Guidelines | Air disinfection, water purification, disinfection of articles and ventilation | |
| Interim Guidance for SARS-CoV-2 Testing in Non-Healthcare Workplaces | Testing for SARS-CoV-2 | |
| Classification standard for epidemic prevention for keeping social distance | South Korea | Social distance, wearing masks, limiting the number of people entering and gathering in public places, and suspending the operation of some public facilities |
| Grading standard for epidemic prevention response | Social control | |
| IMMUNE Building Standard | Belgium | Architectural engineering, technology, design and operational practices |
| Guidance Infection prevention and control for seasonal respiratory infections in health and care settings (including SARS-CoV-2) for winter 2021 to 2022 | Britain | Protective measures such as barrier design / provision of collective ventilation, etc. |
| Guidelines for prevention and control of novel coronavirus (COVID-19) in food production and operation enterprises | Sanitary practices, cleaning and waste disposal, sick staff management, social distance |
SARS-CoV-2: severe acute respiratory syndrome coronavirus 2.
So epidemic protection should take a variety of measures at the same time[5,6], and designing a “safe” space to meet all basic human needs (including epidemic prevention needs) now and in the future has become a key challenge for architects today[7]. In terms of the whole life cycle of building design, operation and service, epidemic prevention should be considered from the planning and design level to improve the epidemic prevention ability of buildings, and the building epidemic prevention standard should be formulated to control the transmission route of COVID-19 from the source and reduce the risk of epidemic infection, so as to achieve the same purpose as the anti-seismic standard, aimed at reducing earthquake damage and improving the anti-seismic ability of buildings.
Therefore, by summarizing the current research standards of building epidemic prevention, including the status, problems and prospects of building epidemic prevention, the paper puts forward the importance of establishing standards of building epidemic prevention, and the content of epidemic prevention should be added to building design disaster prevention system. Simultaneously, the systematic idea of residential building epidemic prevention design is introduced providing an effective and feasible reference and enlightenment for the formulation of normalization standards for global epidemic prevention of building.
2. Methods
A systemic review is carried out, focusing on improving the epidemic prevention capacity of the building and reducing its impact on the transmission of epidemic diseases in the building during COVID-19. Systematic methods are used for research identification and selection to improve the evaluation quality and evidence.
2.1 Aim
The purpose of this study is to summarize the relationship between epidemics (such as COVID-19, SARS, etc.) and building environment, discuss and study what epidemic prevention measures can be taken in buildings to reduce the risk of epidemic virus transmission in buildings, and find out the design scheme that can improve the epidemic prevention ability of buildings by analyzing the influencing factors of building epidemic prevention.
2.2 Inclusion and exclusion criteria
Inclusion criteria include research on epidemic diseases (such as COVID-19, SARS, etc.) and healthy buildings. The transmission of virus, building environment, transmission route of virus, influencing factors of virus transmission and prediction of the number of infected people are considered, and the papers obviously irrelevant to building epidemic prevention were manually removed.
Regarding COVID-19 and building epidemic prevention, the norms, standards and guidelines on COVID-19 and the peer review were screened from January 1, 2020 to August 12, 2022.
2.3 Search strategy
Literature retrieval is carried out in the Web of Science database. Additional searches were conducted on the websites of World Health Organization and the Centers for Disease Control and Prevention (CDC), and national prevention and control policies and guidelines were searched through Google and Baidu. The literature included in the manual search study and its category percentage are shown in Table 2.
Table 2. Transforming infrastructure.
| Categories | ||||||
| Keywords | Medicineand Biology | Environmental Sciences | Infectious Diseases | Computer Science | Building | Others |
| COVID-19 | 24.45% | 7.70% | 5.88% | 2.12% | 2.88% | 56.97% |
| SARS-CoV-2 | 22.27% | 3.28% | 9.62% | 1.74% | 1.05% | 62.04% |
| Epidemic prevention | 12.21% | 5.80% | 13.75% | 5.58% | 2.32% | 60.34% |
| Building epidemic prevention | 9.09% | 5.07% | 16.70% | 8.67% | 6.77% | 53.70% |
| Epidemic prevention standard | 19.74% | 5.18% | 11.65% | 9.71% | 3.24% | 50.48% |
SARS-CoV-2: severe acute respiratory syndrome coronavirus 2.
The retrieval strategy uses a combination of the following terms: COVID-19 (154,176), SARS-CoV-2 (67,324), epidemic prevention (6,413), building epidemic prevention (473) and epidemic prevention standards (309). The search results are divided into five categories: Medicine and Biology, Environmental Sciences, Infectious Diseases, Computer Science, Building and Others. Among them, there are still very few studies on building epidemic prevention and its standards, accounting for less than 0.3% of COVID-19. And no matter what kind of keyword, less than 7% of the research related to architecture.
2.4 Study selection
In order to carry out this research more accurately, after searching all relevant literature, the documents needed were screened in two stages, and all the documents were retrieved by a librarian (expert searcher) trained in systematic reviews. In stage 1, the titles and abstracts of all references related to architecture and epidemic prevention were reviewed by 2 reviewers and 1 statistician (meta-analysis), and those works and abstracts that appeared to meet the inclusion criteria were selected, and the rest were excluded (in case of disagreement, the decision will be made by the first author). In stage 2, the same selection criteria were applied to the full-text articles to confirm these studies, and finally the papers available for this study were selected to support the following, carefully analyzed by all authors.
3. Problems and Prospects for Epidemic Prevention of Building
3.1 Anti-epidemic measures and existing problems
The current measures to deal with COVID-19 are mainly to prevent the spread of the epidemic, rather than precaution. The current measures are mainly passive protective measures taken after the spread of the epidemic, including quarantine, blockade, travel restrictions, contact tracking, limiting social distance and wearing masks, etc. Although vaccination has also been taken as an active means of epidemic prevention, with the promotion of vaccination, many people are still infected after the whole process of vaccination, indirectly proving that vaccination can’t completely block the spread of the epidemic in a good way[8]. From the perspective of building design, epidemic prevention measures of building may control the spread of the virus from the source before the virus is detected. However, due to differences in economic level and culture, different countries have adopted different epidemic prevention and control measures.
China’s prevention and control measures have basically succeeded in blocking the spread of the epidemic[9-11]. Currently China’s epidemic transmission pressure mainly comes from overseas input. Therefore, China has mainly adopted the epidemic prevention policy of “travel restriction and Dynamic Zero-COVID policy”. Travel restrictions mainly prevent the influx of imported cases from abroad, while other low-risk cities in China can gradually lift the blockade[12]. The “Dynamic Zero-COVID policy” has well solved the problem of local outbreaks and does not affect the development of other cities. Facts have proved that the “Dynamic Zero-COVID policy” has achieved good success in exchange for China’s overall stability and prosperity with minimal economic cost and small-scale public health intervention measures.
Singapore[13] adopts an active preventive strategy without blocking communities and restricting mobility, but actively tracking and isolating close contacts with confirmed patients through post hoc activities, so as to eliminate the source of infection and keep the scale of infection at all times controllable.
Europe and the United States have adopted a limited public health management and mass immunization mode, resulting in mass immunization through natural immunization[14-17]. However, with the emergence of mutant strains (such as Omicron), this method has brought great hidden dangers. The United States[17] has called for mass immunization mode since the beginning of the epidemic, and the CDC issued new epidemic prevention guidelines on February 25, 2022, that is, 70% of Americans may not wear masks, maintain social distance and stay away from the crowded places[15]. But after the new year of 2022, the United States diagnosed more than one million cases on a single day in January 3rd, while the United Kingdom also diagnosed on a single day in January 4th, reaching a new high of 200 thousand cases.
Comparing the epidemic prevention and control measures of China, Singapore, South Korea, to that of the United States and Europe, the current prevention and control modes of various countries are mainly divided into two modes. One is the prevention and control mode represented by China, which is to cut off the transmission route of the virus and reduce the continuous spread of the virus in the population as much as possible until the virus is barely detected. The other is the limited management and group immunization mode proposed by Europe and the United States, especially the United Kingdom.
According to the anti-epidemic policies of China, South Korea and other countries, most of the measures are passive and extensively mandatory measures for the spread of the epidemic, in which there may be some problems. Kissleret et al. pointed out that one-time social distance measures reduced the epidemic peak of transmission free from seasonal compulsion[18]. For the typical viral load and infection dose of SARS-CoV-2, if you only keep a social distance, even if you keep 3 m between two speakers, the upper limit of infection risk after a few minutes is 90%. Wearing masks can significantly reduce the infection efficiency, when both wear fit FFP2 masks, the upper limit of infection risk after 1 hour is 0.4%[19]. Koo et al.[20] found that isolation measures are very effective only in relatively mild outbreaks (i.e. they are very effective in small-scale outbreaks with local outbreaks in the context of relatively controlled outbreaks like China), while the effect is much lower in the context of large-scale outbreaks in severe cases. For example, when the epidemic in China just broke out, and the epidemic in Singapore continued to deteriorate after relaxing epidemic prevention measures, etc.
Whether it is the European and American model or the Chinese epidemic prevention model, taking strict public health intervention measures is not a long-term remedial measure to limit the spread of COVID-19. Therefore, it is essential to research building design based methods and scientific prevention and control means to reduce the spread of infectious diseases.
3.2 Epidemic prevention of building
Many pandemics in history had resulted in inestimable economic losses and casualties. After SARS, many researches on epidemic prevention were applied to buildings. After the outbreak of COVID-19 epidemic, scholars and researchers from different industries launched research on epidemic prevention. The current research is mainly for the post-outbreak of the epidemic. In fact, scholars suggested long time ago to achieve epidemic prevention by improving the building environment based on building design. In 1939, the Athens Charter pointed out that modern cities should coordinate the problems of residence and transportation closely related to people’s lives. In 1981, the International Union of Architects pointed out that the discipline of architecture should enter the era of environmental health, focus on “residence and health”, and consider the three aspects of “building-human-environment” as a whole[21]. Studies have found that the contact distance between residents will have a significant impact on the diffusion of respiratory droplets, thus affecting the efficiency of existing ventilation strategies[22-24], which can effectively dilute and/or remove pollutants in the air[25-28]. Improving ventilation can effectively control the diffusion path of virus and other pollutants and therefore reduce the risk of infection[29-31]. However, under the adverse outdoor air environment, the use of natural ventilation will lead to the outdoor air carrying virus entering the room, increasing the risk of infection. When mechanical ventilation is used, the virus and bacteria attached to the filter screen will be brought into the room, causing further pollution. Therefore, ventilation is the main measure to optimize the indoor air environment of the building, but it also has potential health risks[32,33].
The study on building epidemic prevention is still less and not comprehensive enough, but many basic research related to epidemic prevention is crucial for the future epidemic prevention design of building, which mainly focuses on three directions:
• Using artificial intelligence method, combining epidemiological model with medicine to study epidemic prediction, virus transmission monitoring, diagnosis and treatment, vaccine development and drug testing;
• Looking for CO2 and other media to characterize the spread direction of the virus, so as to evaluate the infection risk of the virus and predict the transmission risk and scope of the virus;
• Through CFD and other numerical simulation methods, study the transmission and diffusion mechanism of influenza virus and other pollutants and the methods to improve building design, so as to dilute the concentration and reduce the transmission risk of virus and other pollutants.
3.3 Epidemic prevention related standards
After 2014, the United States released many standards of WELL series[34,35], and classic ASHRAE standards[36-38] paid more attention to thermal comfort, ventilation and energy-saving measures in buildings. After 2016, China successively issued the Assessment standard for healthy building[39]. These standards are committed to improving the health attributes of building and enhancing the health security of residents, but there is no specific design standard for epidemic prevention of building against influenza. The traditional standard for healthy building takes into account the thermal comfort, ventilation and energy-saving measures in the built environment, but not the epidemic prevention design. Compared with the residents in ordinary buildings, people have not been spared in healthy buildings either through COVID 19 pandemic. There is no obvious gap of the infection risk of residents between both. Meanwhile, the current buildings have not been designed to effectively combat the spread of infectious diseases[40].
Therefore, with the outbreak of COVID-19, China has issued several industrial and local standards related to COVID-19 epidemic prevention, mainly aimed at improving epidemic prevention and control system, environmental hygiene requirements, personal hygiene protection, cold-chain food requirements, current limiting measures and emergency measures, so as to control the spread of the epidemic as soon as possible. These massive epidemic prevention guidelines may be one of the reasons for controlling the infectious diseases rapidly in China. Also, the United States has issued relevant epidemic prevention standards, such as Interim Guidance for SARS-CoV-2 Testing in Non-Healthcare Workplaces. South Korea has issued epidemic prevention standards such as Classification standard for epidemic prevention for keeping social distance, further refined and classified social distance restriction measures in accordance with the degree of epidemic spread. Health by Design Building Institute in Belgium released IMMUNE Building Standard in June 2021, aiming to adopt 135 measures to assess and certify its resilience to withstand present and future health challenges, and minimize the impact of a pandemic and other bacteriological or toxicological threat[41].
The standard system of building epidemic prevention has not been formed at the national, industry, local, and enterprise levels. Table 1 shows some standards directly related to epidemic prevention.
Regretfully, after the outbreak of the epidemic, various countries issued various standards for epidemic prevention measures to deal with COVID-19, but these standards are all in the late stage of control after the outbreak. So far, there is still a lack of building standards for epidemic disasters, and there is no complete epidemic prevention design standard of building around the world, and no early control method to reduce the transmission risk of infectious sources from the building level[3].
Therefore, for the construction of buildings in the post epidemic era, it is necessary to pay extra attention to the epidemic prevention safety of long-term residential and public buildings for work and study[2]. In the meanwhile, putting forward to the new spatial indicators and standards related to epidemic prevention from building design[40,42]. From the whole life cycle of building design, operation and service, the planning and design of epidemic prevention at the building level, the establishment of building epidemic prevention standards and the improvement of building epidemic prevention capacity are of great significance for the prevention and reduction of epidemic spread in the future.
3.4 Epidemic prevention design standard
As the first systematic building standard focusing on epidemic prevention control from the architectural level, the Epidemic prevention design standard of residential building[43] constructed a system of residential space environment, supporting facilities, medical and health services and property services with epidemic prevention function, not only to prevent the spread of respiratory infectious diseases (such as COVID-19, SARS, influenza, etc.) through aerosol, droplet, contact and other means of transmission in residential buildings, but also reduce the impact on residents health and society.
The framework of epidemic prevention design standard of residential building is shown in the Figure 1. The standard also innovatively defines three epidemic prevention levels for residential buildings according to vulnerability, user aggregation density and immunity (refer to Section 4.1). In order to facilitate the architectural designer to integrate epidemic prevention into each special design of architectural design at the beginning of design, the standard guides the epidemic prevention design of the building from the whole life cycle, including Site and General Plan, Building, Heating, Ventilation and Air Conditioning System, Water supply and drainage, Intelligence, Medical and Health Services, Operation and Maintenance, so as to ensure the epidemic prevention ability of building space design, building internal facilities, water supply and drainage, ventilation and so on.
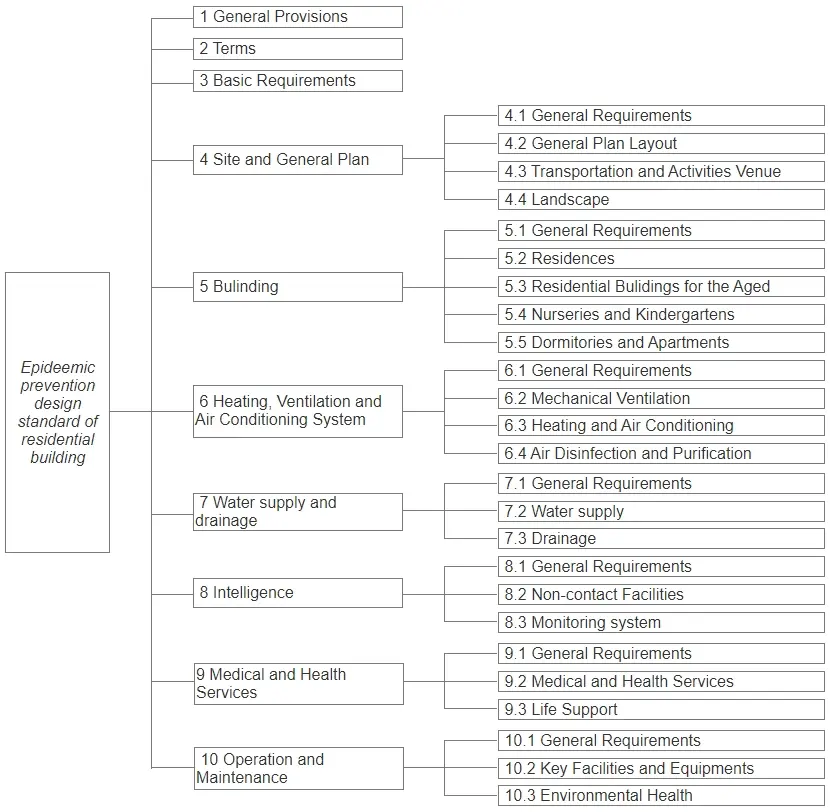
Figure 1. The framework of epidemic prevention design standard of residential building[43].
3.5 Application effect of building epidemic prevention
Although the design standards for building epidemic prevention have not been issued, many buildings have adopted some epidemic prevention facilities and building means to reduce the spread of the epidemic under the background of the continuous variation of SARS-CoV-2 and the continued severe COVID-19 epidemic.
The current epidemic prevention design is mainly aimed at the epidemic prevention transformation of existing buildings to reduce the risk of contact transmission and air transmission.
In order to cope with covid-19, Ligao Junyu Garden community in Shenzhen carried out epidemic prevention transformation in 2021 and established a property epidemic prevention system, mainly adopting measures to reduce contact and purification, such as setting contactless gate, face recognition door opening, elevator epidemic prevention purifier, garbage room purifier, etc. The effect is that there are no infected people in the community and successfully resisted several outbreaks in Shenzhen since 2021. In addition, the original terminal D of Shenzhen airport was transformed for epidemic prevention in 2021, mainly aiming at the transformation of air conditioning and ventilation system and health management system, so as to ensure that there is no mixed flow between aircrew and passengers, increase the function of ventilation, purification and disinfection, and reduce the cross transmission of air. Since then, there has been no epidemic spread in Shenzhen airport proving to a certain extent that epidemic prevention transformation can reduce the spread of epidemic virus.
At the beginning of 2022, Omicron attacked Shenzhen. The “0215” epidemic situation in Shenzhen shows that the use of some epidemic prevention equipment can reduce the spread of the epidemic in the community to a certain extent. According to the data of Shenzhen Municipal Health Commission, a total of 1,156 people were infected in Shenzhen, of which 706 lived in Futian District, accounting for 61.07% of the total number of infected people. Among the infected people in Futian District, 399 (56.52%) lived in Village-in-city in Shenzhen, and the remaining 307 were distributed in 80 districts. The spread of the “0215” epidemic in Shenzhen mainly occurred in Village-in-city. After infection cases were found in each Village-in-city, the epidemic spread rapidly and on a large scale. The infection status of the six Village-in-cities with the largest number of infections in Shenzhen is shown in Table 3. However, there was no large-scale spread after the infection cases were found in the community, and the number of infected people was basically in the range of 1-8. According to the survey, most of the Village-in-cities with infection have poor infrastructure conditions, dense population and buildings, small building spacing, poor ventilation environment and high risk of transmission between buildings. Therefore, it is easy to cause large-scale spread infection after the emergence of infection sources. On the contrary, the community buildings have large spacing and good ventilation conditions, and are now equipped with non-contact epidemic prevention facilities such as face recognition and takeout boxes, greatly reducing the risk of contact. Therefore, after the emergence of infection sources in the community, the transmission rate is low, and there is no community diffusion.
Table 3. Infection status of six village-in-city with the largest number of infections in Shenzhen[44].
| Village-in-city | Number of infected persons | Community communication time |
| 1 | 173 | 27 |
| 2 | 59 | 24 |
| 3 | 45 | 24 |
| 4 | 26 | 23 |
| 5 | 13 | 10 |
| 6 | 12 | 8 |
4. Discussion
The three aspects of infection source control, ventilation and air purification are considered to be used for building epidemic prevention to reduce the spread of virus and the concentration of virus in the air, so as to reduce the concentration of virus inhaled by residents. Although the current standards related to epidemic prevention provide relatively comprehensive guidelines for measures such as environmental hygiene, personal protection, isolation, quarantine, movement restriction, and community intervention, several issues remain in the epidemic prevention design of buildings. The standard basis, epidemic prevention products, design modes, and epidemic prevention and control platforms are discussed in detail in Section 4.1 to Section 4.4.
Section 4.1 to Section 4.4 are the main research direction and difficulty of building epidemic prevention at present, and also the main content of epidemic prevention design standards of building. These aspects are taken into account in building planning and design, effectively reducing the risk of virus transmission in the building[25-28]. And quantifying building epidemic prevention measures to reduce the risk of virus transmission in buildings is also an important research direction in the future.
4.1 Epidemic prevention grade and risk assessment of building based on vulnerability
Vulnerability in the paper refers to vulnerable people’s susceptibility and the state of having little resistance to environmental or social change and lack of adaptive capacity[45]. Different living groups have different needs for building design, the indoor environments designed for the majority might be risky for the vulnerable groups. Therefore, the epidemic prevention design standard of building should fully consider groups with different vulnerabilities, especially vulnerable groups, such as the elderly, children, commuters and workers. China’s “Epidemic prevention design standard of residential building” defines three epidemic prevention grades of design based on vulnerability for residential buildings:
Grade I: applies to high-populated buildings for people with weak immunity such as nurseries, kindergartens, where serious epidemic consequences might occur. Other residential buildings with special requirements applies, too.
Grade II: applies to medium-populated buildings for people with physical dysfunction or weak immunity, such as the elderly.
Grade III: applies to buildings for people living in groups with strong immunity.
First of all, since children’s immune systems are not yet mature and their ability to take care of themselves is weak, nurseries, kindergartens and other children’s places are defined as the Grade-I epidemic prevention of design, which is the highest epidemic prevention level. Secondly, due to the deterioration of the immune system, the elderly are vulnerable groups, most of whom can take care of themselves, though. Therefore, the buildings where the elderly mostly live are defined as the Grade-II epidemic prevention of design. In other cases, the buildings can follow the normal epidemic prevention design. While vulnerable groups such as long-term exposed commuters and staff have their presence in all buildings, targeted epidemic prevention measures are taken in each epidemic prevention level.
Compared with fire and earthquake disasters, pandemics such as the COVID-19 have a wider area of harm and greater economic and social impact. However, it is difficult to quantify the risk assessment of pandemics such as COVID-19 and SARS, etc., and no relevant epidemic prevention design standards of building have been issued to guide the design of building so far. Due to technical and time limit, the area of the epidemic is large, and the epidemic monitoring indicators are difficult to quantify the risk of transmission and spread. Not only the type and characteristics of the virus, but also indicators such as exposure duration and infection rate must be determined.
Therefore, architects or researchers should take epidemic prevention into consideration, balancing the epidemic prevention of building with the susceptibility of vulnerable groups under the guideline of “reducing the risk of transmission through design”, which is not only helpful for COVID-19 prevention, but also for improvement of buildings to prevent the spread of epidemics.
4.2 Epidemic prevention products for buildings
With the outbreak of the epidemic, the demand for epidemic prevention products such as masks and respirators, is gradually increasing. At present, epidemic prevention products related to buildings mainly include air purifiers, face recognition, automatic temperature measurement, epidemic prevention and disinfecting products of buildings (public toilet sanitary disinfecting products, elevator disinfecting machines, etc.). Epidemic prevention materials for building mainly disinfected and sterilized by blocking air transmission and contact transmission. Excellent epidemic prevention products for buildings can prevent virus when used in places with poor ventilation and high risk of transmission by reducing the transmission of the virus in the building.
The virus can be transmitted through air, surface contact, water and other ways inside the building. Therefore, many areas inside the building may be high-risk areas for infection. For example, the elevator may be considered a high-risk area for infection due to its small space area and high use frequency. Therefore, products to prevent air transmission which are able to quickly purify the air in a very short time, should be placed in the elevator and thus preventing the virus from infecting the current and subsequent elevator passengers. Moreover, areas with high contact frequency such as elevator buttons and door handles are high-risk areas of contact transmission. Therefore, epidemic prevention products that can quickly kill viruses, such as nanofilm, should be used. In addition, for regarding water transmission inside the building, the technology to prevent the floor drain from drying up and the air flow in the water pipe should be adopted to prevent the aerosol from spreading to other rooms through the water pipe.
The use of air purifiers can significantly reduce the contact between aerosols and droplets[46], reduce aerosol exposure by 31%-66%. With the increase of air flow, the exposure and dependence on source location will be reduced[47], and effectively dilute virus carrying aerosols[48]. However, current purification products mainly use HEPA filter screens to intercept the virus and have a short service life and inconvenient replacement. Although it can reduce the risk of virus transmission to a certain extent, it mainly plays the role of filtering rather than killing the virus in the actual application scenario. If it is not replaced in time, the virus will multiply and may cause secondary pollution. Moreover, the blockage of the filter in the air purifier or the age of the equipment will affect the effectiveness of the air purifier[49,50]. Therefore, when using the air purifier for epidemic prevention, it is recommended to replace or clean the filter at a higher frequency than the ordinary use frequency. And the air outlet of the air purifier can change the flow field of indoor air, thus changing the path of virus diffusion, reducing the accumulation of pollutants, and reducing the risk of indoor transmission.
In addition to air purifiers for buildings, it is of great significance to develop epidemic prevention materials that can be combined with buildings. For example, epidemic prevention materials can be applied not only to elevator buttons, door handles and other places with high contact frequency to block the way of virus transmission, but also to water pipes and floor drains to block the transmission of virus carrying aerosols through water pipes and floor drains, and also to air purifiers, fresh air fans, air conditioners, exhaust fans and other products to quickly sterilize. In particular, it should be applied to the elevator epidemic prevention purifier in the elevator car, so as to meet the purpose of rapid virus killing in the elevator.
Therefore, the development of epidemic prevention products for buildings should follow several principles: good combination with buildings, fast sterilization, fast identification and fast alarm.
4.3 Design mode-healthy wind environment in buildings
The epidemic prevention design of buildings should be based on the whole life cycle, but the current building design mode does not combine many building technologies well. Diluting virus concentration through ventilation is recognized as an effective method to reduce the risk of virus transmission. The epidemic prevention design of the building should be designed by CFD and epidemiology in the design stage, so as to optimize the design of the building community and house type according to the simulation results and ensure the good ventilation of the community and house type, and to block the route of virus transmission, increase epidemic prevention facilities and reduce the risk of virus transmission in the design stage.
The existing standards mainly organize the air flow through thermal comfort, but rarely through the diffusion of viruses and other pollutants. Even if there is enough fresh air, it cannot ensure that the virus can be diluted to a concentration that is not infectious in time in the indoor and outdoor space. Therefore, the healthy wind environment in the building needs to evaluate the ventilation efficiency in combination with the air distribution index and building characteristic index. Specifically, the indicators to be combined with the healthy wind environment of the community include roads, window opening direction, building spacing, accessibility of infectious sources, air diffusion, etc., while combined with the healthy wind environment of the house type including air age, removal efficiency, accessibility of air supply, accessibility of infectious sources, energy utilization coefficient, air diffusion performance uneven coefficient of air distribution, etc. Designers shall design the layout of buildings, roads, windows, balconies, toilets, etc. according to the aerodynamic characteristics and the temporal and spatial distribution of viruses and other pollutants in the air[51]. Airflow affects the sedimentation and diffusion of virus and other pollutants[52,53]. Not only can proper ventilation and good outdoor air prove to reduce the transmission of indoor pollutants and viruses through the air[54], but also reasonable building space organization will effectively reduce the transmission of viruses in the community[55].
Advanced ventilation design tools such as computational fluid dynamics (CFD), should be integrated into virus diffusion and risk assessment models. In the background of COVID-19, it is feasible to design healthy ventilation based on CFD simulation using more targeted methods[56].
In the future, COVID-19 and other respiratory epidemics will be simulated by CFD in the building community and indoor to find out the propagation rules and paths, so as to optimize the layout and apartment layout. CFD is used to simulate the possible diffusion paths of virus carrying aerosols and virus carrying droplets in the environment where the building is located, so as to give the best location and orientation of the building monomer, water supply and drainage pipeline design, ventilation equipment, equipment layout location, sidewalk width and route, pedestrian travel route, etc. However, this requires long-term epidemiological data and in-depth pathological research.
4.4 Epidemic prevention and control platform
Compared with most natural disasters, the epidemic caused by SARS-CoV-2 lacks early warning, prediction and prevention and control system. It has typical interpersonal characteristics, wide spread range, no definite physical boundary restrictions, and even the “trans-provincial and transnational” spatial spread is like[57,58]. In the future, in response to the dilemma of uncertain disasters and epidemic outbreaks (which may occur at any time), the construction of buildings and even cities may expose many deficiencies in planning, design and operation.
Therefore, in order to improve the ability of buildings to deal with the epidemic caused by COVID-19 in the future, the epidemic prevention standards should be established to improve the epidemic prevention for buildings. After the implementation of epidemic prevention design in building planning and design and building products, the epidemic prevention requirements should also be implemented in the process of building operation. Especially when epidemic has occurred, the implementation of good health intervention measures, home isolation, nucleic acid detection and disinfection measures were found to be very important. Therefore, a normalized epidemic prevention and control platform should be established to uniformly manage, monitor, detect and treat the epidemic before, during and after the occurrence of the epidemic, so as to efficiently organize the epidemic prevention work and improve the epidemic prevention ability of building operation.
Therefore, it is essential to break through the barriers between monitoring, detection, tracking, medical treatment and flow regulation and form a unified epidemic prevention and control platform with real-time monitoring, rapid detection, rapid tracking, rapid diagnosis and treatment and rapid response to health and measures of epidemic prevention. And, to achieve a comprehensive epidemic prevention and control platform, multidisciplinary research still needs to be deeply integrated, including epidemiology, medicine, architecture, big data, internet of things, rapid prediction model, etc.
5. Conclusions
This paper reviews the status of epidemic in the interior of building, the current anti-epidemic measures and epidemic prevention related standards, and comes to the conclusion that the current buildings are still insufficient in the design of effectively resisting the spread of infectious diseases, and there is no standard guideline in the building design for epidemic prevention so far. Therefore, by considering the epidemic prevention design in the architectural planning and design stage, the use of building epidemic prevention products, healthy wind environment design, etc. to establish a healthy building environment can effectively reduce the risk of epidemic transmission inside the building. The paper puts forward the significance of formulating building epidemic prevention standards, which has a long way to go. In-depth and multidisciplinary research should be carried out in the study of epidemic prevention. And more, we should accumulate long-term epidemiological data and pathological research of epidemic hazards such as SARS-CoV-2, and formulate appropriate epidemic prevention standards of building and evaluation methods.
Since we spend most of our time in enclosed buildings including home, schools, offices and other indoor spaces, the health consequences of building design, epidemic transmission and daily epidemic prevention must be comprehended. As described in the paper, the construction industry must address some challenges and research opportunities to better understand the impact of the epidemic virus on buildings and residents. In order to achieve effective epidemic prevention of building, we must have an overall and interdisciplinary research framework through which experts in architecture, medicine, data science, artificial intelligence and other disciplines cooperate in coordinated efforts, so as to connect the parameters related to buildings, residents and epidemic diseases, to establish common standards and frameworks and assess how buildings are designed to support epidemic prevention and health.
Although the Epidemic prevention design standard of residential building has been prepared and applied in new residential projects, the construction cycle of buildings is generally long, so the effectiveness of the standard still needs long-term follow-up research, and the content of the standard still needs to be tested in practice. And based on operational conditions, quantifying epidemic prevention measures can reduce the risk of virus transmission in buildings.
Acknowledgements
The authors are grateful to other main drafters of this standard: Zhong Jishou, Cheng Xinhong, Jiang Xing, Lin Yang, Wan Heng, Zhou Xiaoqing, Liu Jian, Liu Wenjie, Pan Yungang, Ding Lixing, Xu Xuesong, Shi Xuan, Cui Dongjin, Chen Sitian, Meng, Wang Yi, Gao Xudong, Wang Xiaodong, Wang Hongchao, Lin Chaonan, Wu Yongsheng, Ding Puxian, Yu Peng, Yuan Jixin, Sou Zhihong, She Yong, Huo Xiaoping, Gan Quan.
Authors contribution
Lei Y, Bu Z, Gong X: Conceptualization, methodology, analysis, writing original draft.
Cai Y: Writing, review, editing.
Conflicts of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
Not applicable.
Funding
This research is financially supported by Practical Research on Low Carbon and Healthy Building System in Fujian and Guangdong for China Construction Fangcheng Investment& Development Group Co., Ltd. (CSCECFC-2022-KJZX--06), Research on Intelligent System of Healthy Residential Buildings for Smart Building Research Center of China Real Estate Association, and Research and Verification of Epidemic Prevention System of Residential Buildings (Shenzhen science and technology plan project in engineering construction field in 2021).
Copyright
© The Author(s) 2022.
References
-
1. Harapan H, Itoh N, Yufika A, et al. Coronavirus disease 2019 (COVID-19): A literature review. J Infect Public Health. 2020;13(5):667-673.[DOI]
-
2. Wang J. Vision of China’s future urban construction reform: In the perspective of comprehensive prevention and control for multi disasters. Sustain Cities Soc. 2021;64:102511.[DOI]
-
3. Gong X, Liu J, Wu L, Zhu Z. Development of a healthy assessment system for residential building epidemic prevention. Build Environ. 2021;202:108038.[DOI]
-
5. Magnavita N, Chirico F. Headaches, Personal Protective Equipment, and Psychosocial Factors Associated With COVID‐19 Pandemic. Headache. 2020;60:1444-1445.[DOI]
-
6. Magnavita N, Sacco A, Nucera G, Chirico F. First aid during the COVID-19 pandemic. Occup Med. 2020;70(7):458-460.[DOI]
-
7. Glavan OL, Nikolić N, Folić B, Vitošević B, Mitrović A, Kosanović S. COVID-19 and City Space: Impact and Perspectives. Sustainability. 2022;14(3):1885.[DOI]
-
8. Heidari A, Navimipour N, Unal M, Toumaj S. The COVID-19 epidemic analysis and diagnosis using deep learning: A systematic literature review and future directions. Comput Biol Med. 2022;141:105141.[DOI]
-
9. Tang B, Wang X, Li Q, Bragazzi NL, Tang S, Xiao Y, et al. Estimation of the transmission risk of the 2019-nCoV and its implication for public health interventions. J Clin Med. 2020;9(2):462.[DOI]
-
10. Tang B, Bragazzi NL, Li Q, Tang S, Xiao Y, Wu J. An updated estimation of the risk of transmission of the novel coronavirus (2019-nCov). Infect Dis Model. 2020;5:248-255.[DOI]
-
11. Kong X, Liu F, Wang H, Yang R, Chen D, Wang X, et al. Prevention and control measures significantly curbed the SARS-CoV-2 and influenza epidemics in China. J Virus Erad. 2021;7(2):100040.[DOI]
-
12. Xiang Y, Jia Y, Chen L, Guo L, Shu B, Long E. COVID-19 epidemic prediction and the impact of public health interventions: A review of COVID-19 epidemic models. Infect Dis Model. 2021;6:324-342.[DOI]
-
13. Ministry of Health, Singapore [Internet]. Infection prevention and control guidelines and standards. Singapore: Ministry of Health, Singapore; [cited 2022 March 10]. Available from: https://www.moh.gov.sg/hpp/all-healthcare-professionals/guidelines/GuidelineDetails/infection-prevention-and-control-guidelines-and-standards
-
14. Brglez M, Udovič B, Maček A. Covid-19 and the European Parliament (policies): a Year of Periloues Ad-hoc Solutions. J Comp Polit. 2021:14(2):81-97. Available from: https://www.proquest.com/openview/e55fc51b7da6ac09f116d5739dcd6b3d/1?pq-origsite=gscholar&cbl=426376
-
15. Centers for Disease Control and Prevention. COVID-19 global response strategy [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; [cited 2022 March 23].
-
16. Engler S, Brunner P, Loviat R, Loviat R., Abou-Chadi T, Leemann L, Glaser A, et al. Democracy in times of the pandemic: explaining the variation of COVID-19 policies across European democracies. West Eur Polit. 2021;44(5-6):1077-1102.[DOI]
-
17. Li M, Colby H. Association between actual and perceived US COVID-19 policies and preventive behavior. Ann Behav Med. 2021;55(4):369-375.[DOI]
-
18. Kissler SM, Tedijanto C, Goldstein E, Grad YH, Lipsitch M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science. 2020;368(6493):860-868.[DOI]
-
19. Bagheri G, Thiede B, Hejazi B, Schlenczek O, Bodenschatz E. An upper bound on one-to-one exposure to infectious human respiratory particles. Proc Natl Acad Sci U.S.A. 2021;118(49):e2110117118.[DOI]
-
20. Koo JR, Cook AR, Park M, Sun Y, Sun H, Lim JT, et al. Interventions to mitigate early spread of SARS-CoV-2 in Singapore: a modelling study. Lancet Infect Dis. 2020;20(6):678-688.[DOI]
-
21. Liang HZ. Development and quality evaluation of healthy housing. [dissertation]. Taiyuan (China): Taiyuan University of Technology; 2004.
-
22. Villafruela J, Olmedo I, José JS. Influence of human breathing modes on airborne cross infection risk. Build Environ. 2016;106:340-351.[DOI]
-
23. Liu L, Li Y, Nielsen PV, Wei J, Jensen RL. Short-range airborne transmission of expiratory droplets between two people. Indoor Air. 2017;27(2):452-462.[DOI]
-
24. Cortellessa G, Stabile L, Arpino F, Faleiros DE, van den Bos W, Morawska L, et al. Close proximity risk assessment for SARS-CoV-2 infection. Sci Total Environ. 2021;794:148749.[DOI]
-
25. Li Y, Leung M, Tang JW, Yang X, Chao CY, Lin JZ, et al. Role of ventilation in airborne transmission of infectious agents in the built environment-a multidisciplinary systematic review. Indoor Air. 2007;17(1):2-18.[DOI]
-
26. Nielsen PV. Control of airborne infectious diseases in ventilated spaces. J R Soc Interface. 2009;6(suppl 6):S747-S755.[DOI]
-
27. Morawska L, Tang JW, Bahnfleth W, Bluyssen PM, Boerstra A, Buonanno G, et al. How can airborne transmission of COVID-19 indoors be minimised? Environ Int. 2020;142:105832.[DOI]
-
28. Kissler SM, Tedijanto C, Goldstein E, Grad YH, Lipsitch M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science. 2020;368(6493):860-868.[DOI]
-
29. Li YG. Engineering control of indoor transmission of infectious diseases-movement of droplets and ventilation control. In: Progress in new technologies of refrigeration and air conditioning. Proceedings of the Third Symposium on new technologies of refrigeration and air conditioning, 2005. p. 18-22.
-
30. Zhao B, Zhang Z, Li X. Comparison of biological particles distribution in different ventilated rooms. Heat Vent Air Cond. 2003;33(03):37-40.
-
31. Jiang Y, Zhao B, Li X, Yang X, Zhang Z, Zhang Y. Investigating a safe ventilation rate for the prevention of indoor SARS transmission: An attempt based on a simulation approach. Build Simul. 2009;2(4):281-289.[DOI]
-
32. Wen Y, Leng J, Shen X, Han G, Sun L, Yu F. Environmental and health effects of ventilation in subway stations: a literature review. Int J Environ Res Public Health. 2020;17(3):1084.[DOI]
-
33. Ding L, Zha X, Deng K, Yan H. Wet-processing characteristics and inactivation dynamics model of indoor air microorganisms under air-conditioning system. Refrig Air-Cond. 2015;15(10):90-94. Chinese. Available from: https://kns.cnki.net/kcms2/article/abstract?v=NK8hpUzgeRVBaUAeXFzeIWv3tP4PMOfxZvG3qqgzw7NZ80_L08aI3uTLaiL6T6JW_S1sGMSXBEqTpY5jk4Wh7Gi2YoSo9bDklWCpjiWwv9Y2eoJCEm_yinaYs8QU5O7voFV2W_qASaxV5k89LtVftaMznw5MY2dFODwltjKBMtDpzAokr51rNELB9pN7cmVy&uniplatform=NZKPT&language=CHS
-
34. International WELL Building Institute [Internet]. WELL Building Standard v1.0. New York: International WELL Building Institute. Available from: https://well.support/well-building-standard-v1~6f796447-4851-474d-b7dd-5caa76125654
-
35. International WELL Building Institute [Internet]. WELL v2™. New York:International WELL Building Institute. Available from: https://v2.wellcertified.com/en/wellv2/overview
-
36. ASHRAE [Internet]. Standard 90.1: Energy Standard for Buildings Except Low-Rise Residential Buildings. Atlanta (GA): ASHRAE; [cited 2022 April 24]. Available from: https://www.ashrae.org/technical-resources/bookstore/standard-90-1
-
37. ASHRAE [Internet]. ASHRAE/ANSI Standard 55-2010 Thermal Environmental Conditions for Human Occupancy. Atlanta (GA): ASHRAE; 2010 [cited 2022 May 2]. Available from: https://www.lorisweb.com/CMGT235/DIS06/ASHRAE-55-2010.pdf
-
38. ASHRAE [Internet]. Standards 62.1 & 62.2: Ventilation for Acceptable Indoor Air Quality. Atlanta (GA): ASHRAE; [cited 2022 June 4]. Available from: https://www.ashrae.org/technical-resources/bookstore/standards-62-1-62-2
-
39. China Academy of Building Research, Chinese Society For Urban Studies, China Architectural Design & Research Group. Assessment standard for healthy building: T/ASC 02-2016. Beijing: Archit Soc China; 2017.
-
40. Awada M, Becerik-Gerber B, Hoque S, O’Neill Z, Pedrielli G, Wen J, et al. Ten questions concerning occupant health in buildings during normal operations and extreme events including the COVID-19 pandemic. Build Environ. 2021;188:107480.[DOI]
-
41. Healthy by Design Building Institute (HDBI). The IMMUNE Building Standard [Internet]. Brussels (BE): Healthy by Design Building Institute; 2020 [cited 2021 Feb 28]. Available from: https://immune-building.com/certification/
-
42. Navaratnam S, Nguyen K, Selvaranjan K, et al. Designing Post COVID-19 Buildings: Approaches for Achieving Healthy Buildings. Buildings. 2022;12(1):74.[DOI]
-
43. China Association for Science and Technology. Announcement on the latest developments in science and technology [Internet]. Beijing: China Association for Science and Technology; [cited 2022 June 4]. Available from: http://english.cast.org.cn/
-
44. Shenzhen Municipal Health Commission [Internet]. COVID-19 daily update. Shenzhen (China): Shenzhen Municipal Health Commission; [cited 2022 June 4]. Available from: http://wjw.sz.gov.cn/yqxx/content/post_9639496.html
-
45. O’Lenick CR, Wilhelmi OV, Michael R, Hayden MH, Baniassadi A, Wiedinmyer C, et al. Urban heat and air pollution: A framework for integrating population vulnerability and indoor exposure in health risk analyses. Sci Total Environ. 2019;660:715-723.[DOI]
-
46. Chen C, Zhao B, Cui W, Dong L, An N, Ouyang X. The effectiveness of an air cleaner in controlling droplet/aerosol particle dispersion emitted from a patient’s mouth in the indoor environment of dental clinics. J R Soc Interface. 2010;7(48):1105-1118.[DOI]
-
47. Castellini JE Jr, Faulkner CA, Zuo W, Lorenzetti DM, Sohn MD. Assessing the use of portable air cleaners for reducing exposure to airborne diseases in a conference room with thermal stratification. Build Environ. 2022;207:108441.[DOI]
-
48. Dai H, Zhao B. Reducing airborne infection risk of COVID-19 by locating air cleaners at proper positions indoor: Analysis with a simple model. Build Environ. 2022;213:108864.[DOI]
-
49. Rodríguez M, Palop ML, Seseña S, Rodríguez A. Are the Portable Air Cleaners (PAC) really effective to terminate airborne SARS-CoV-2? Sci Total Environ. 2021;785:147300.[DOI]
-
50. Zhao B, Liu Y, Chen C. Air purifiers: A supplementary measure to remove airborne SARS-CoV-2. Build Environ. 2020;177:106918.[DOI]
-
51. Yao J, Zhang H, Liu X, Wang Y. Numerical simulation of the influence of air distribution on indoor particle matter distribution. Procedia Eng. 2017;205:3405-3412.[DOI]
-
52. Chen H, Feng Z, Cao SJ. Quantitative investigations on setting parameters of air conditioning (air-supply speed and temperature) in ventilated cooling rooms. Indoor Built Environ. 2019;30(1):99-113.[DOI]
-
53. Zhang Y, Yu W, Li Y, Li H. Comparative research on the air pollutant prevention and thermal comfort for different types of ventilation. Indoor Built Environ. 2020;30:1092-1105.[DOI]
-
54. William MA, Suárez-López MJ, Soutullo S, Ahmed AA, et al. Evaluating heating, ventilation, and air-conditioning systems toward minimizing the airborne transmission risk of Mucormycosis and COVID-19 infections in built environment. Case Stud Therm Eng. 2021;28:101567.[DOI]
-
55. Yu IT, Li Y, Wong TW, Tam W, Chan AT, Lee JH, et al. Evidence of airborne transmission of the severe acute respiratory syndrome virus. New England J Med. 2004;350(17):1731-1739.[DOI]
-
56. Cao SJ. Challenges of using CFD simulation for the design and online control of ventilation systems. Indoor Built Environ. 2019;28(1):3-6.[DOI]
-
57. Nadim SS, Chattopadhyay J. Occurrence of backward bifurcation and prediction of disease transmission with imperfect lockdown: A case study on COVID-19. Chaos Solitons Fractals. 2020;140:110163.[DOI]
-
58. Kraemer MUG, Yang CH, Gutierrez B, Wu CH, Klein B, Pigott DM, et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science. 2020;368(6490):493-497.[DOI]
Copyright
© The Author(s) 2022. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Publisher’s Note
Science Exploration remains a neutral stance on jurisdictional claims in published
maps
and institutional affiliations. The views expressed in this article are solely those
of
the author(s) and do not reflect the opinions of the Editors or the publisher.
Share And Cite



Science Exploration Style
Gong X, Yuan L, Bu Z, Cai Y. ADDIN CNKISM.UserStyleStandards and problems for epidemic prevention in buildings: a review. J Build Des Environ. 2023;1:6202. https://doi.org/10.37155/2811-0730-0101-4
Tips
Copy completed.
Submit a Manuscript
Author Instructions
Cite this Article
Article Metrics
0
View
0
Download
Cited
Article Updates

- Abstract
- Keywords
- 1. Introduction
- 2. Methods
- 3. Problems and Prospects for Epidemic Prevention of Building
- 4. Discussion
- 5. Conclusions
- Acknowledgements
- Authors contribution
- Conflicts of interest
- Ethical approval
- Consent to participate
- Consent for publication
- Availability of data and materials
- Funding
- Copyright
Science Exploration Style
Gong X, Yuan L, Bu Z, Cai Y. ADDIN CNKISM.UserStyleStandards and problems for epidemic prevention in buildings: a review. J Build Des Environ. 2023;1:6202. https://doi.org/10.37155/2811-0730-0101-4
copy
Share Link
copy