A comprehensive analysis of factors influencing the selection of indoor air quality improvement solutions for healthcare projects in Vietnam
Dang Nguyen Hong Anh
1
,
Ahn Yong Han
2

,
Thach Nguyen Thao
1
,
Mohamed S. A. Binyumen
3
,
Pham Duy Hoang
4,*
*Correspondence to:
Pham Duy Hoang, Center for Ai Technology in Construction, Hanyang University, Gyeonggi-do, Ansan 15588, Republic of Korea.
E-mail: phamduyhoang@hanyang.ac.k
J Build Des Environ. 2024;2:28343. 10.37155/2811-0730-0302-10
Received: January 17, 2023Accepted: April 10, 2024Published: May 06, 2024
This article belongs to the Special lssue Towards Net Zero Energy Mass Custom Homes and Communities
Abstract
Vietnam battles severe air pollution and substandard infrastructure, leading to sick building syndrome (SBS), even in healthcare facilities. Enhancing indoor air quality (IAQ) in hospital design and renovations is vital for safeguarding vulnerable groups, such as patients, children, and the elderly. However, akin to other developing nations, Vietnam must address specific local challenges before devising any strategies to improve IAQ in these critical settings. In this study, we identify factors influencing the selection of methods to improve IAQ in healthcare facilities, considering Vietnam’s specific conditions. 16 potential factors have been investigated and categorised into 4 influence groups based on a comprehensive literature review and validated by a survey of 160 architects, engineers, project managers, and hospital staff. We conducted an academic literature review to pinpoint these factors and propose design solutions. Additionally, we surveyed and quantified the effects from the perspective of Vietnamese healthcare experts. Based on our findings, we discussed the impact of these factors and suggested solutions for enhancing IAQ during the design and renovation phases of hospitals. The study’s contribution lies in its practical insights for stakeholders seeking to improve IAQ. The outcomes of this study aim to provide a foundation for developing guidelines and standards to assess construction quality in healthcare facilities.
Keywords
Factor analysis, indoor air quality, healthcare project, green specification
1. Introduction
Indoor air quality (IAQ) plays an essential role in healthcare settings, profoundly affecting both patient outcomes and the well-being of healthcare staff. A hospital building is a uniquely built environment because its primary function is maintaining and restoring health, but it also carries the potential risk of spreading infectious diseases. Poor IAQ is known to affect the health and well-being of building occupants and has been linked to sick building syndrome (SBS), which refers to a collection of chronic illnesses such as headaches, irritation of the eyes, nose, and throats, or dry and itchy skin[1]. The SBS prevalence for healthcare workers at a large-scale hospital is 70.1% in Ho Chi Minh City, a metropolitan with an average annual air quality index of 87 US AQI and PM2.5 concentrations four times higher than the WHO guidelines[2]. Poor IAQ is also associated with an increased risk of hospital-required infection, of which respiratory infections are the most common, accounting for up to 80% of cases in Vietnam hospitals[3]. Some causes of infections are viruses, mold in the air, and medical equipment contaminants. Specific contaminants’ sources in hospital environments vary, including emissions from building materials, heating and cooling systems, electronic equipment, and occupant activities[4]. Moreover, healthcare facility air often contains particles and gaseous pollutants, such as carbon dioxide, formaldehyde, volatile organic compounds, and bacteria. The study by Keyvani et al. illustrates the complex interaction between external and internal factors affecting hospital IAQ, underscoring the importance of maintaining good indoor air standards to mitigate the risks posed by airborne pollutants and ensuring a safe and healthy environment[5].
Several factors must be taken into account when considering IAQ improvement measures in hospital wards, including the adoption of advanced technologies and management in-depth evaluation, as evidenced by case studies from countries like China, Italy, Portugal, Spain, Thailand, and Nigeria[6-10]. For instance, in China, Liu et al. investigated the quality of the indoor environment in two healthcare facilities by using an integrated instrument to calculate objective physical environment and subjective satisfactory survey[6]. Settimo et al. have outlined existing guidelines for IAQ in hospital settings in Europe, offering valuable frameworks[7]. Farraia et al. investigated the influence of legislation on hospital air quality in Portugal, mainly focusing on the installation of high-efficiency particulate arrestance (HEPA) filters in patient rooms and analysing the resultant air quality changes pre- and post-legislative implementation[8]. In Vietnam, different strategies to enhance IAQ have been implemented incoherently, such as centrally controlled ventilation systems and in-room air purifiers. There is insufficient research on improving IAQ in Vietnamese healthcare projects owing to a lack of public awareness and a database to complete national regulation, revealing the need for alternative strategies for stakeholders.
Sustainable construction practices, including green building (GB) strategies, are recognized as effective solutions for hospital wards to perform better than conventional buildings in terms of IAQ performance, energy use, and occupant satisfaction[10]. According to Chung, Vietnamese hospitals, often housed in buildings from the 1900s, face issues with aging structures and limited renovation options. Additionally, Vietnam’s hospital design standards and guidelines predominantly focus on functional and structural aspects, often overlooking air quality considerations. This neglect is also evident in the ratio of IAQ credits in Vietnam’s green building guidance systems. However, due to economic and infrastructural gaps, Vietnam and other developing countries struggle to apply advancements in improving hospitals’ IAQ. Quang points out that many public hospitals (which constitute 94% of Vietnam’s healthcare system) have ventilation issues in surgical rooms and hallways, failing to meet the national standard TCVN 4470:2012. In contrast, private hospitals adhering to international standards like WELL and AACI report significantly lower hospital-acquired infection rates. However, it is limited in quantity and only available in developed cities. These contrasts underscore the urgent need for Vietnam to update its healthcare design standards, ensuring effective and high-quality healthcare. In addition to the national system, hospitals voluntarily certified by GB standards can utilise three strategies-emission source control, ventilation, and IAQ measurement guidelines-to enhance IAQ, save energy, reduce recovery times, and boost staff productivity[11]. The LEED-compliant LOTUS framework in Vietnam incorporates national regulations QCVN alongside international standards like ASHRAE 62.1, AS 1668, and European Standards EN 779 and EN 1822, setting comprehensive IAQ criteria[12,13]. Additionally, Fitwell and the WELL Building Standard, focusing on health and wellbeing, complement BREEAM standards. These guidelines are primarily tailored for projects in developed countries, where conditions for improving IAQ-including cognitive, technical, and financial aspects-are favourable.
Therefore, our study investigates these factors through a literature review and a questionnaire survey involving 160 construction industry professionals. We employed factor analysis to assess the influence of various variables. The goal was to identify and prioritize the key factors that significantly impact the choice of IAQ improvement methods in Vietnamese hospital projects in line with sustainable construction goals and healthcare requirements.
2. Literature Review
As the global healthcare system becomes more sophisticated, people’s requirements for the healthcare environment become more stringent, and it is essential to build an indoor environment that satisfies the occupants. IAQ, thermal, visual, and acoustic environments belong to indoor environmental quality (IEQ) in survey research and are considered the highest priority in choosing a healthcare building[14]. Retrofitting has been identified as a key approach to improving energy efficiency and IAQ in hospital buildings Radha[15]. As emphasized by several studies, the importance of good IAQ in hospitals underscores the need for targeted research in this area. Furthermore, Hiwar et al. provide a quantitative analysis of the relationship between airborne microorganisms and indoor air distribution in hospitals[16]. Rodrigo et al. highlight the importance of maintaining the indoor atmosphere in reducing hospital-acquired infections in developing countries, emphasizing its importance in healthcare settings[17]. Ratajczak explores ventilation strategies in nursery buildings during COVID-19, with findings applicable to enhancing IAQ in hospitals[18]. These studies underscore its critical impact on health outcomes in healthcare environments and the need for effective management strategies. Stockwell et al. discuss how ventilation affects bioaerosols, pointing to the necessity of evaluating the effectiveness of ventilation systems in controlling IAQ and bioaerosol concentrations[19]. Brittain et al. connect high ambient air pollution with increased mortality from viral diseases, indicating the need to explore how ambient pollution influences air and viral outbreaks in hospital settings[20]. Lastly, Ikhtiar discusses reducing microbial counts through improved ward ventilation, highlighting the need for research on specific ventilation strategies and their effectiveness in controlling microbial levels[21]. Olsson and Hansen discussed the viewpoints of project management, owner, and contractor and prioritised user involvement in project design for achieving flexibility in hospital projects[22]. From the perspective of the hospital manager, Ibrahim et al. published the determinants of hospital IAQ, including contextual factors, building design, operation factors, and occupant-related factors[23]. The framework serves as a foundation for our selection of surveyors from hospital staff, and atmosphere-influencing variables must be effectively understandable throughout the occupancy. Collectively, these studies reinforce the complex interplay of various factors affecting the quality of indoor air in hospitals and the need for comprehensive research from the design stage to develop effective strategies for improvement.
The barriers and challenges hindering IAQ and green construction technology are becoming more prevalent in developing markets. According to Pitt’s research in 2009, sustainable construction can be driven by focusing on drivers and barriers, methods and techniques, and benchmark indicators. Recent research has inherited this approach for investigating their locals. A study conducted in Kuwait[24] carried out a questionnaire survey to assess the level of comprehension of GB among construction stakeholders. Educational programs and legal frameworks are perceived as drivers and strategies to foster sustainable construction, whereas insufficient knowledge and the absence of governmental incentives represent significant obstacles. Husain utilised the Green-Lean-Six Sigma hierarchy model to investigate the interconnections between barriers and validated them using expert surveys conducted in Pakistan[25]. The inquiry uncovered that the unstable political situation posed a significant hindrance, compounded by the lack of governmental support and client experience. Nguyen conducted an exploratory study on obstacles to the advancement of GB in Vietnam[26]. The author categorised the 41 barriers into four components preventing GB adoption: Socioeconomic and cognitive barriers, Economic and cost barriers, Legislative and institutional barriers, and Technical and knowledge barriers while revealing that the highest mean score indicator is slow policymaking and lack of comprehensive policy. A different study categorised twelve obstacles to advancing sustainable housing in Australia into four categories: economic factors, technical and design factors, sociocultural factors, and institutional factors[27].
The literature review shows that barriers to incorporating IEQ into building designs include a lack of integrated design teams, which ranked the highest in appearance, high initial costs, a poor market for IEQ buildings, and higher design charges, among others[28]. In delivering advanced heating, ventilation, and air-conditioning in buildings, the general fear of higher investment costs compared to conventional buildings is often seen in empirical studies[29,30]. The higher upfront cost of implementing IAQ improvement alternatives represents a significant consideration in the healthcare sector, where budgets are often constrained. Nevertheless, it is crucial to recognise that the initial investment in indoor quality improvements can result in long-term savings by reducing healthcare-associated infections, patient complications, and operational costs and improving healthcare workers’ job satisfaction[19]. Facilitating the promotion and adaptation of suitable present-day innovations in developing countries and enhancing technology transfer between neighbouring countries can reduce the transfer price for technology[31]. IAQ controls success in a hospital and relies on the joint efforts of the engineering, healthcare, administrative, and support staff. Prior research has demonstrated that IEQ management needs an integrated team from the beginning of a project and continuing support during occupancy[32]. ASHRAE’s guideline proposed a concept of an IAQ-integrated design approach for the steering committee, including inclusive design team leaders (architects, engineers, and project managers) with innovations encouraged by clients[23]. Due to continuous operation, healthcare facilities consume over twice as much energy per square as other commercial facility types. However, environmental impacts can be mitigated through renewable energy transition and energy-efficient ventilation systems[33]. These drivers and barriers address critical IAQ concerns and align with broader sustainability goals. The need for strategic planning and advocacy becomes evident as various studies across different countries reveal obstacles such as inadequate knowledge, absence of governmental incentives, economic factors, and the perception of higher upfront costs, emphasising the importance of a comprehensive approach to promoting better IEQ in healthcare settings.
To compensate for the lack of research and building data in the Vietnamese market, we decided to restrict our assessment to factors related to the decision-making process for indoor air solutions. We reviewed existing literature on new technology adoption and design factors that affect the quality of indoor air in healthcare projects. These factors include drivers and barriers to adopting technology from the design and construction manager’s viewpoint. Furthermore, building factors affect the IAQ during operation from a healthcare facility viewpoint. Web of Science, Scopus, and Google Scholar were queried with keywords germane to the study (e.g., IAQ factors, drivers and barriers, Vietnam, hospital…). The inclusion criteria consisted of the following: (1) Drivers and barriers in GB/ IEQ technology adoption (from the perspective of project managers and investors…); (2) Strategy for indoor air quality in hospitals (published from the viewpoint of healthcare workers). The list of 22 influencing variables to enhance IAQ in hospitals from the literature review is described in Table S1. The findings from this comprehensive review will serve as a foundation for assessing strategies and implementing effective renovation solutions in Vietnamese hospital buildings.
3. Research Methods
3.1 Research framework
This document sought to gain a comprehensive insight into the perspectives of industry professionals on integrating influence factors in indoor air quality design in the context of industrial construction in Vietnam. To effectively address the research goal described in the introduction, this study used the following research methods: (1) extensive review of the relevant literature; (2) questionnaire development; (3) dissemination and collection of a structured questionnaire survey; and (4) rigorous data analysis and discussion. The research was mainly focused on examining the existing practices of influence factors in IAQ design among industry practitioners and their perceptions of the general advantages and potential contributions of innovative design solutions. It should be noted that this research does not address specific benefits and challenges associated with each technology. Detailed descriptions of the specific methodologies used are given in Figure 1.
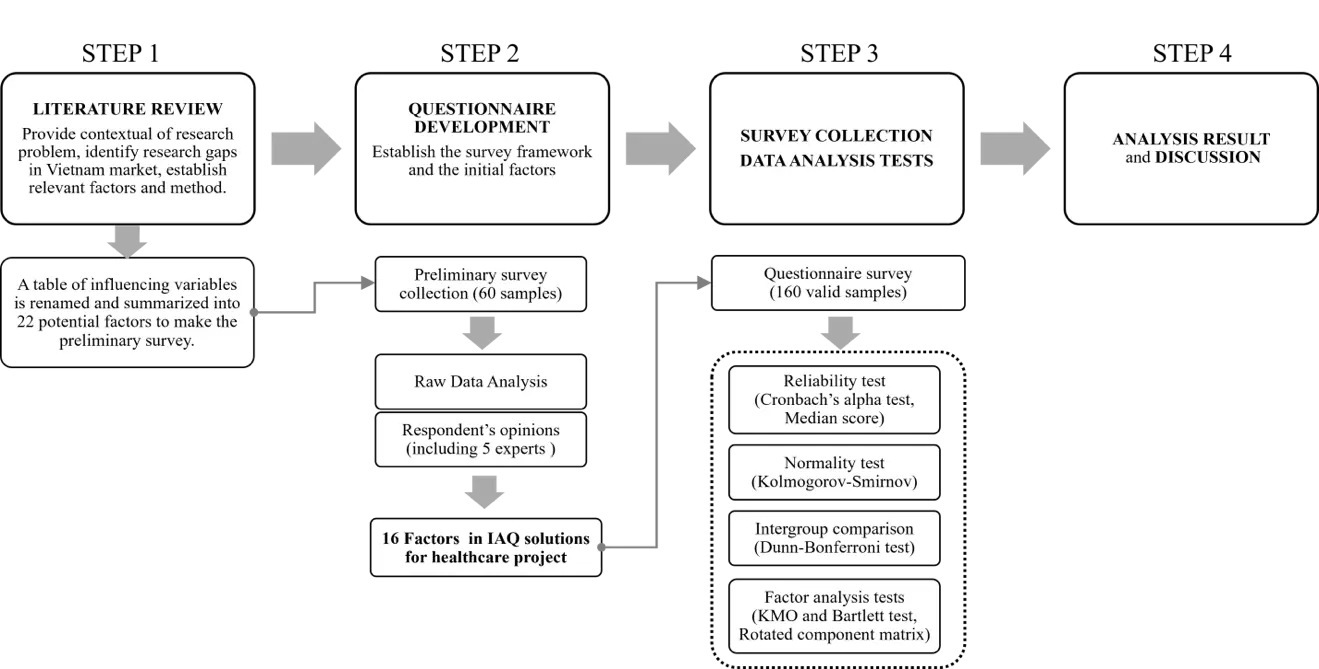
Figure 1. The framework of the paper’s research methodology.IAQ: indoor air quality; KMO: Kaiser-Meyer-Olkin.
3.2 Questionnaire development
3.2.1 Factor identification
We compiled a variety of factors, such as hospital-related requirements, building-related risks, and institutional obstacles, which are associated with the decision-making of construction managers in IAQ design specifications. The pilot inquiry focused on collecting data to develop the survey instrument by reviewing scholarly literature and consulting industry experts. The preliminary survey had 60 interviewees ranked 22 potential variables (Table S1) and then commented on the questionnaire organisation, design, and the comprehensibility of the description. The survey results were validated by Cronbach’s alpha, factor analysis tests, median ranking analysis along with the opinions of 5 industry experts; consequently, 22 evaluated variables were updated, clarified, and synthesised into sixteen impact factors, as analysed in Table 1.
Table 1. Factors influencing the adoption of indoor air quality solutions in the design stage.
| Code | Factors | Clarification |
| D-1 | Project Scale and Planning | • Project scale, site assessment, number of beds, specialities, and Planning of subdivisions, landscapes, and chains affecting the indoor environment. |
| D-2 | Design purpose | • Design goal (human health/energy efficiency) determines the interest and percentage of funds for total IEQ. • The Pre-design phase decides on the specialists needed and the technical approach plan for IAQ. |
| D-3 | SD | • Complexity of project design, assignment to construction specification. • Effective ventilation must be included in architectural, interior, landscape, structural, MEP, and HAVC drawings. |
| D-4 | Outdoor issues and regional environment | Including Physical, Biochemical, and Microclimate around the building area. • The need for data collection for Air Quality Index, water sources, geology, and organisms… |
| E-1 | Initial cost | • Cost of design and operation of the team. • Cost of equipment purchase, transportation, and installation. • Hiring a third party (for executive design and certification test, modelling IAQ). • Certification registration fee. |
| E-2 | Operating/maintenance cost | • Life cycle costing of devices and additional building cost. • Annual maintenance cost for IAQ system and devices. |
| E-3 | Technology transfer cost | • Cost of technology transfer or purchase; fees for technical support and training; intellectual property rights by product or by year. |
| G-1 | Owner’s requirement | • Each hospital project has specialities; depending on the client’s awareness, they can make specific IEQ requirements. |
| G-2 | Commercial advantages | • Financial/ non-financial incentives, attracting investment and loan opportunities. • Opportunities for cooperation and sponsorship from sustainable funds. • Increase competitiveness and raise branding awareness as a marketing tool |
| G-3 | Future legislation | • Need policy understanding, regularly updated standards, and ready for policy and market change. • IAQ tools are flexible and adaptable for future legislation, including the development of construction technology, renewable energy plans, etc. |
| G-4 | Administration | • Requires highly qualified managers and management strategy for building systems. • Stakeholders’ experience and communication ability. |
| T-1 | Feasibility | • Capable of installation in accordance with current engineering techniques and construction conditions. • Simple to install by local workers and straightforward for material suppliers. |
| T-2 | Operability | • Demand for pollution measurement data and usage behaviour collecting. • Demand for a database of material, technology, and products thoroughly. |
| T-3 | Integrated capability | • Need an integrated design team and interoperability between tools; manage the effect of IA system installation on other engineering systems (HVAC-IAQ-Lighting-Acoustics-Fire-Communications, Plumbing, Mechanical, etc.). |
| T-4 | Compatible with medical function | • The system must guarantee that it does not interfere with the hospital’s medical needs, as well as the medical examination and treatment machinery and equipment. |
| T-5 | Emissions level | The impact of IAQ solutions on total building energy consumption, operating and demolition emissions, and environmental impact. |
IAQ: indoor air quality; IEQ: indoor environmental quality; HAVC: heating, ventilation, and air-conditioning; MEP: mechanical, electrical and plumbing; SD: Schematic Design.
3.2.2 Survey collection
Based on the result of the pilot study, the survey was published on Google Form Survey and emailed to collect perspectives from industry consultants of various sizes who are exposed to construction activities and have adequate industry knowledge to contribute to the study. The first part outlined the study’s objectives, briefly introducing sustainable concepts, factors influencing the indoor air quality design process, and specific requirements for the hospital project. The second part asked for basic background information about respondents, including the type of company, occupation, and working experience. The section also included multiple-choice questions that collect respondents’ understanding of past hospital projects (e.g., Have you participated in hospital construction projects? What types of factors have you accepted?). The type of question included a single choice, multiple choice, and text input. In the third part of the survey, respondents were asked to assess the current level of importance and the expected level of investment for each factor in the design phase individually using a five-point scale (1 = Very low, 2 = Low, 3 = Medium, 4 = High, 5 = Very High). Target respondents included Architecture consultant and design contractor (Architect), On-site engineering and construction contractor (Engineer), Building owner and Project management contractor (Manager), Healthcare professionals, and hospital staff (Hospital staff). The individual respondents and companies were from metropolitans in different parts of Vietnam. By asking participants to send the survey to their colleagues, Snowball sampling was used in the questionnaire survey to approach a group of people who work in the hospital and construction industry. The respondents’ demographic information provides an overview of the distribution of construction workers (Table 2). Among valid responses, the background of the respondents that we collected indicated that the survey result was reliable. This information allowed researchers to classify respondents into subgroups for further comparison analysis.
Table 2. Demographic background of respondents and hospital involvement.
| Demographic characteristics | Frequency n = 160 | Valid Percent (%) | |
| Industry firms | Architecture consultant and design contractor | 86 | 53.75 |
| On-site engineering firm and construct contractor | 40 | 25.00 | |
| Building owner and Project management contractor | 15 | 9.37 | |
| Healthcare professionals and Hospital staff | 19 | 11.88 | |
| Years of experience | Less than 2 years | 38 | 23.75 |
| 2 - 5 years | 59 | 36.87 | |
| 5 - 10 years | 29 | 18.13 | |
| More than 10 years | 34 | 21.25 | |
| Hospital project scale involvement | Large general and specialised hospital (> 1000 beds) | 18 | 11.25 |
| Medium general and specialised hospital (250-1000 beds) | 21 | 13.13 | |
| Small general and specialised hospital (< 250 beds) | 5 | 3.13 | |
| Clinics and nursing centres | 11 | 6.87 | |
| None | 105 | 65.62 | |
3.3 Data analysis process
Respondents were asked to assess the important factors influencing indoor air quality design. As described in Figure 1, several statistical methods have been implemented for analysing the collected rating scores, including Cronbach’s alpha, the Kolmogorov-Smirnov test, the Dunn-Bonferroni post-hoc test, and factor analysis. These tests were used to answer the research question (What are the key factors influencing the selection of methods to improve IAQ?). Then, Factor analysis was employed to interpret the underlying adoption factors. The Dunn-Bonferroni test results of intergroup comparisons examine the impact of a company’s backgrounds and career profiles on adopting IAQ solutions. The appropriateness and duration of the tests are presented below.
Median score and Standard deviation were used to measure the level of importance of all items. In the 5-point evaluation scale, the importance level of the factor is recorded as having a value from 3 to 5. In addition to the overall analysis, it is necessary to examine whether respondents’ perspectives from different companies or positions are different and their concerns. The application of parametric statistical tests is based on the hypothesis that data is normally distributed, while non-parametric tests do not have such a prerequisite. Therefore, the Kolmogorov-Smirnov test is required to test the data’s normality and determine the intergroup comparison method[34]. If the p-value of the Kolmogorov-Smirnov test is less than 0.05, the data is not normally distributed, and the Dunn-Bonferroni test is used for comparison between groups. Respondents were separated by company type and working experience. In each group, research hypotheses are set that the respective case influences the practitioner’s perceptions. Then, a Dunn-Bonferroni post hoc test will be used to investigate whether there are significant differences in respondents’ ratings in different subgroups. Suppose the p-value generated (i.e., a probability value) is less than 0.05. In that case, the null hypothesis is rejected, and the research hypothesis is supported, which means that there are significant differences in the attitudes of the respondents of the different groups. Factor analysis is a statistical methodology for describing observed correlation variables as factors that may be smaller than observed variables. In previous studies, factor analysis techniques have been used to identify factors associated with potential obstacles to adopting outside residential construction[35]. Measurements of Kaiser-Meyer-Olkin (KMO) and Bartlett spheres focused on determining whether the correlation matrix was an identity matrix to evaluate the feasibility of factor analysis methods. Close KMO values show strong correlations between variables and determine the appropriateness of factor analysis. Bartlett’s spheres test the statistics of KMO vary from zero to one. If the KMO value exceeds 0.5, the sample is considered suitable for factor analysis.
4. Results
4.1 Analysis of respondents’ demographic
A total of 161 responses were collected, with a response rate of 97%. The outlier has been explored and removed from the final 160 valid responses for data analysis. Table 2 summarises the respondents and their organisation profiles. The majority of respondents (53.75%) are from architecture consultant and design contractor firms, followed by on-site engineering firms and construction contractors (25.00%). Their positions and distribution of working experience in the construction industry signify the validity and understanding of principal design regulations. Regarding respondent’s involvement in hospital projects, Table 2 indicates that 34.38% of respondents have worked in a hospital or engaged in hospital design. However, 65.62% of all respondents are aware of IAQ but never participated in a hospital project.
4.2 The data reliability
Cronbach’s is a prerequisite to performing more detailed analysis in previous management studies[36]. This test was used to measure internal consistency in a set of questions. The coefficient is between 0 and 1; the closer the score to 1, the more consistent the practitioner perceives between these Likert scale elements. The reliability test results show that Cronbach’s coefficient of 0.788 in the questionnaire’s adoption factors exceeded the 0.70 thresholds, respectively. Consequently, the results of the Cronbach test confirm the reliability of the data collected for analysis, and other tests can be applied.
The result of the data normalisation test is presented in Table 3. For Kolmogorov-Smirnov tests, the test statistics for all groups (E1, E2, E3, ..., T5) are smaller than 1, indicating that the maximum absolute difference between the empirical distribution function of the sample and the cumulative distribution function of the normal distribution is relatively small. The P-value for all groups is reported as .000 less than the significant level (usually 0.05), indicating a rejection of the null hypothesis of normality. Therefore, non-parametric tests should be conducted for subsequent data analysis. The median value for all factors (D1 to T5) is consistently 4, suggesting that, on average, respondents perceive each factor as equally influential in selecting IAQ solutions. This uniformity in median values implies a consensus among respondents regarding the significance of these factors. Moreover, the standard deviation values for each factor range from 0.623 to 0.827 (below 1), indicating relatively low variability in respondents’ perceptions across all factors. This demonstrates the credibility of the survey and factors list, emphasising a comprehensive approach to considering different factors during the design process.
Table 3. The result of the normality test and factors’ median value.
| Factors | Kolmogorov-Smirnova | Min | Max | Median | Std. Deviation | ||
| Statistic | df | Sig. | |||||
| D1 | .244 | 160 | .000 | 1 | 5 | 4 | 0.776 |
| D2 | .252 | 160 | .000 | 1 | 5 | 4 | 0.758 |
| D3 | .264 | 160 | .000 | 1 | 5 | 4 | 0.810 |
| D4 | .251 | 160 | .000 | 1 | 5 | 4 | 0.820 |
| E1 | .263 | 160 | .000 | 1 | 5 | 4 | 0.742 |
| E2 | .275 | 160 | .000 | 1 | 5 | 4 | 0.664 |
| E3 | .275 | 160 | .000 | 1 | 5 | 4 | 0.709 |
| G1 | .262 | 160 | .000 | 1 | 5 | 4 | 0.707 |
| G2 | .274 | 160 | .000 | 1 | 5 | 4 | 0.694 |
| G3 | .252 | 160 | .000 | 1 | 5 | 4 | 0.700 |
| G4 | .314 | 160 | .000 | 1 | 5 | 4 | 0.623 |
| T1 | .243 | 160 | .000 | 1 | 5 | 4 | 0.771 |
| T2 | .247 | 160 | .000 | 1 | 5 | 4 | 0.764 |
| T3 | .267 | 160 | .000 | 1 | 5 | 4 | 0.753 |
| T4 | .259 | 160 | .000 | 1 | 5 | 4 | 0.827 |
| T5 | .289 | 160 | .000 | 1 | 5 | 4 | 0.758 |
a: lilliefors significance correction.
4.3 Intergroup comparison
The Kolmogorov-Smirnov test results indicate that all variables have P-values below 0.05, which means that data is not normally distributed, and that the Dunn-Bonferroni post hoc test should be used to compare between groups. Respondents are divided into different groups according to various types of companies and work experience. Variables with p-values less than or equal to 0.05 are considered statistically significant, indicating the differences rated and/or perceived among different professional backgrounds. The results of the Dunn-Bonferroni post hoc test for intergroup comparisons are also shown in Table 4. Notably, variables with p-values marked by asterisks (*), such as D1, G2, and T1, exhibit statistically significant differences in median value among the company types. These considerable differences imply that Architects, Engineers, Managers, and Hospital Staff hold distinct perspectives on these factors in the hospital project. Upon scrutinising the results derived from the Dunn-Bonferroni test, discernible statistical distinctions emerge among the examined groups, denoted by the presence of asterisks signifying statistical significance. Within the variable of “Industry firm”, noteworthy disparities are observed in several instances. Specifically, in variable D1, the “Manager” subgroup stands out significantly (P = 0.014), suggesting a risk-averse attitude among managers. By prioritising design, regulatory compliance, and cost, Managers address key risk factors associated with IAQ investment in the project. In variable G2, the “Engineer” and “Hospital staff” exhibit notable divergence (P = 0.005*). Furthermore, variable T1 indicates significant differentiation, with the “Hospital staff” subgroup once again showcasing distinctiveness (P = 0.048*), emphasising their particular role in shaping IAQ solution adoption dynamics.
Table 4. Factor intergroup comparison.
| Variables | Industry firm | Post hoc | Experience year | Post hoc | ||||||
| Architect | Engineer | Manager | Hospital staff | < 2 years | 2-5 years | 5-10 years | > 10 years | |||
| D1 | 4 | 4 | 5 | 4 | 0.014* | 5 | 4 | 4 | 4 | 0.010* |
| D2 | 4 | 4 | 4 | 4 | 0.532 | 4 | 4 | 4 | 4 | 0.760 |
| D3 | 4 | 4 | 4 | 4 | 0.369 | 4 | 4 | 4 | 4 | 0.506 |
| D4 | 4 | 4 | 4 | 4 | 0.606 | 4 | 4 | 4 | 4 | 0.221 |
| E1 | 4 | 4 | 4 | 4 | 0.056 | 4 | 4 | 4 | 4 | 0.293 |
| E2 | 4 | 4 | 4 | 3 | 0.476 | 4 | 4 | 4 | 3 | 0.411 |
| E3 | 4 | 4 | 4 | 3 | 0.727 | 4 | 4 | 3 | 4 | 0.673 |
| G1 | 4 | 4 | 4 | 4 | 0.158 | 4 | 4 | 4 | 4 | 0.519 |
| G2 | 4 | 3 | 4 | 3 | 0.005* | 4 | 4 | 4 | 3 | 0.261 |
| G3 | 4 | 4 | 4 | 3 | 0.074 | 4 | 4 | 4 | 3 | 0.801 |
| G4 | 4 | 4 | 4 | 3 | 0.449 | 4 | 4 | 4 | 4 | 0.247 |
| T1 | 4 | 4 | 4 | 3 | 0.048* | 4 | 4 | 4 | 3 | 0.468 |
| T2 | 4 | 4 | 4 | 3 | 0.101 | 4 | 4 | 4 | 3 | 0.404 |
| T3 | 4 | 4 | 4 | 3 | 0.201 | 4 | 4 | 4 | 4 | 0.643 |
| T4 | 4 | 4 | 4 | 3 | 0.072 | 4 | 4 | 4 | 4 | 0.134 |
| T5 | 4 | 3 | 4 | 3 | 0.123 | 4 | 4 | 4 | 3 | 0.702 |
*: The mean is significant at the 0.05 level of significance.
Moreover, regarding the variable of “Experience year”, the “< 2 years” subgroup also prioritises the design requirements factor D1 (P = 0.010*), implying nuanced IAQ solution adoption tendencies within this cohort. The attention given to design by less experienced groups could result from less learning from established practices or guidelines. Additionally, variables E2, G2, G3, T1, T2, T5 reveal that the “> 10 years” subgroup tends to underestimate factors compared to the others. Although this difference is not significantly distinct, it underscores potential disparities in IAQ solution implementation strategies among individuals with long experience levels. The project team has much experience, which is attributed to the success of optimising the infrastructure design of hospital construction[37]. In this subgroup of respondents, 31.4% are hospital employees, and 45.7% are from architectural firms. Meanwhile, those with 5-10 years of experience might have witnessed the long-term benefits or challenges of previous IAQ initiatives, reinforcing the importance of design considerations. The insignificant discrepancies in ranking factors indicate that there are no insignificant subgroups or specific issues in the IAQ design process. Recognising these variations and balancing stakeholders’ expertise and priorities should be conducted within an integrated framework to decide the whole design within the context of IAQ from the conceptual design stage to close out.
4.4 Factor analysis result
The high KMO measure and the significant Bartlett’s test are shown in Table 5, indicating a high-quality factor analysis. The variables are well-suited for this analysis, and the factors extracted are likely meaningful. In factor analysis, factor loadings play a crucial role in understanding the relationship between observed variables and underlying latent factors. Table 5 represents variables associated with four group factors: Technology (T), Government (G), Economic (E), and Design (D). The table also includes factor loadings, which range between -1 and 1 and quantify the extent to which each variable is associated with a particular factor. High loadings, especially those close to 1, signify a strong correlation between a variable and its corresponding factor, indicating that the variable is a good representative of the factor’s underlying construct. For instance, T4’s loading of 0.752 on the Technology factor is significant, implying that T4 is a strong indicator of the characteristics or attributes that define the Technology factor. High loadings (e.g., E2 on Factor E with 0.803) suggest that these variables strongly represent the respective factor. Similarly, variables such as G2 and G1 showcase substantial loadings of 0.750 and 0.738, respectively, on the Government factor, highlighting their relevance in capturing the essence of governmental requirements and regulations. However, the variable D2 exhibits a relatively low loading of 0.567 on the Design factor. The survey respondents believe that the hospital project’s design purpose and speciality plan have no impact on the other factors in the Design group when selecting solutions for IAQ.
Table 5. Summary of factor analysis result.
| Code | Extracted factors loadings | ||||
| 1 | 2 | 3 | 4 | ||
| Compatible with medical function | T4 | 0.752 | |||
| Operability | T2 | 0.703 | |||
| Emission loads | T5 | 0.695 | |||
| Integrated capability | T3 | 0.628 | |||
| Feasibility | T1 | 0.623 | |||
| Commercial advantages | G2 | 0.750 | |||
| Owner’s requirement | G1 | 0.738 | |||
| Administration | G4 | 0.696 | |||
| Future Adaptabilities | G3 | 0.650 | |||
| Operating/maintenance cost | E2 | 0.803 | |||
| Technology transfer cost | E3 | 0.798 | |||
| Initial cost | E1 | 0.763 | |||
| Outdoor issues and regional environment | D4 | 0.782 | |||
| Project Scale and Planning | D1 | 0.717 | |||
| Schematic Design | D3 | 0.661 | |||
| Design purpose | D2 | 0.567 | |||
5. Discussion
This paper sought out to answer the question what the primary factors are influencing the selection of methods to improve IAQ. Sixteen critical factors, grouped into economic, governance, design, and technical categories, are discussed below. The results of a Dunn-Bonferroni test comparing groups examining the impact of a company’s background and career profile on adopting IAQ solutions show insignificant differences in perceptions of IAQ and necessitate collaboration among diverse stakeholders. Given Vietnam’s slow update of national standards, uneven contractor development, and limited research, utilising GB tools as guidelines effectively improves IAQ and overall hospital performance. By emphasising project stakeholders’ roles and distinctions, the Indoor Air Quality Guide from ASHRAE[23] proposed a strategy for assembling an integrated design team to achieve good IAQ and sustainable building design. Beyond ventilation control systems, the building structure, operation, and activities significantly impact indoor air quality. Thus, all members of the design team must weigh this possibility, ensuring unified solutions aligned with investor needs and legal requirements. Based on the survey results and recording the opinions of respondents, architects are primarily concerned with the architectural and spatial aspects of projects. They prioritise design-related IAQ factors, including the layout, choice of materials, and overall seamless integrated solutions, increasing users’ experiences. Engineers approach IAQ from a technical and practical standpoint. They focus on the feasibility of the technology and control its long-term maintenance and operation. Project Managers and Hospital staff have a governance-oriented perspective. They focus on compliance with IAQ regulations and standards, considering risk management, and allocating resources effectively, including budget, throughout the life cycle of healthcare facilities. The manager group’s focus on these aspects also indicates strategic planning. By considering design and regulatory compliance, managers are likely aiming for long-term viable solutions, avoiding future modifications or non-compliance penalties. Hospital staff, including medical professionals and facility staff, receive IAQ as part of their health risk and productivity work. They are also concerned about the impact of IAQ on patient outcomes and healthcare operational processes. The findings underscore the multifaceted nature of IAQ improvement plans in hospital projects and how diverse company types and experience levels contribute to differing perceptions and priorities.
5.1 Economic factors
In Vietnam, the focus on initial investment costs (E1) for hospital air quality improvements often overshadows considerations like operating/maintenance costs (E2) and technology transfer costs (E3). Similar to previous studies[26,28] high initial cost risks are one of the top issues when applying new technology to buildings. The added costs and associated risks of unique solutions for IAQ and IEQ in general may discourage initial investors from committing[38]. The primary driver of high initial costs is the need for sophisticated air filtration systems and upgraded ventilation capacities to meet healthcare standards. These improvements, crucial for removing harmful particles such as pathogens and allergens, often involve high-end solutions like HEPA filters and UV-C germicidal irradiation. Such systems are significantly more expensive than traditional domestic suppliers’ standard commercial filters or conventional techniques. Moreover, updating ventilation systems, which includes increasing outdoor air exchange rates and ensuring proper air pressure balance throughout the hospital, adds to the financial burden during operation[39]. This is particularly true for older hospitals, which may require significant structural modifications to accommodate new IAQ systems. The respondents revealed that cost concerns are one of the most significant barriers in IAQ design when developers and contractors are aware of the advantages but are not always ready to pay for the upgraded solutions.
To address these challenges, hospitals in Vietnam can consider several strategies. Implementing IAQ improvements in phases, focusing on areas at greatest risk of airborne infection, such as Patient room, Infectious isolation room, Protective isolation room, Intensive care unit, Delivery room, Laboratory, and Operating/surgical room, can reduce upfront costs. Utilising modular air purification systems, including low-cost monitoring that can be adjusted as needed, offers a cost-effective and flexible solution[9]. Additionally, leasing air quality control equipment, instead of outright purchases, helps spread the financial impact over a more extended period[31]. Forming partnerships with private companies for shared investments can also lessen the financial load on hospitals, making essential air quality improvements more manageable and sustainable.
5.2 Design factors
This factor refers to a project’s “design” and design stages. It contains four variables: “D1” project scale and planning; “D2” design purpose; “D3” schematic design; and “D4” outdoor issue and regional environment. Architectural performance must be set up to meet the primary role, i.e., the health of occupants and patients’ recovery time, follow regulatory standards, as well as minimise the need for future renovations[40]. The results of this study emphasise the need for a structured design process supported by literature, which includes an Initial Assessment and Needs Analysis. This phase involves auditing real-time air quality index, examining ventilation and filtration systems, identifying contamination sources, and engaging stakeholders to align with IAQ standards[41]. The subsequent Goal Setting and Planning phase aims to set measurable air quality improvement objectives, incorporating strategies like upgrading HVAC systems, pressure - humidity - temperature control, improving ventilation methods, adopting advanced air purification, controlling building materials, including finishing and furniture, and green building practices while considering budget and financial viability[19,42]. Designers may ensure IAQ through architectural design by referring to comprehensive guidelines in GB standards such as LEEDs, ASHRAE, and international recommendations[7,12,13]. The survey participants showed that their barrier to an actual project is finding a reliable IAQ professional design unit in Vietnam. Therefore, design-related solutions for complex projects such as entryway systems, ventilation strategy, façade designs, and building envelopes using green materials, e.g., must be discussed between design units to ensure IAQ. The results also raise the need to update traditional design features in Vietnamese hospitals. These conventional design features are no longer suitable for contemporary IAQ standards and healthcare needs. It notes a shift in modern Vietnamese hospital architecture away from outdated designs, such as buildings without entrance systems and carpets that accumulate dirt and microbes. Instead, there is a move towards natural ventilation in areas like patient registration, reflecting a broader trend in updating building designs to meet the evolving healthcare demands and environmental considerations.
5.3 Governance factors
Four variables (“G1” owner’s requirements, “G2” commercial advantages, “G3” future adaptabilities, and “G4” administration) are grouped into the governance strategy factors. The group factor shows the importance of the purpose and governance system of the project based on the local legal framework. However, relative to other factor groups, the Governance factor group is currently underemphasised, reflecting a notable shortfall in attention from governmental and managerial bodies. Compared to studies conducted in developed countries, the primary factor causing delays in hospital projects in Vietnam is the poor ability of owner, management and supervision[43]. The regulatory environment is undeveloped, and the slow decision-making process is considered a high barrier in the Vietnam market[26]. The lack of government incentives is similar to the situation in green building developing markets[44,45]. Evidence from the policy issue, the Guidance for annual hospital quality assessment (Decision 6858/QĐ-BYT) includes 83 criteria to evaluate building facility conditions, human resources qualifications, and healthcare basis.
Insights gleaned from developed economies underscore the importance of government interventions in enhancing the sustainability of the construction sector. This aspect of sustainability encompasses not only the improvement of living conditions within buildings, including aspects like air quality and acoustic comfort but also the broader environmental impact. To advance the IAQ in hospitals, it is imperative that government solutions be implemented. These should include the establishment of guiding standards and mandatory regulations, coupled with supportive measures that span both procedural guidance and financial assistance. Such a comprehensive approach is crucial for improving hospital IAQ significantly, aligning with the best practices observed in more developed economic contexts. Beyond ventilation control systems, the building structure, operation, and activities significantly impact indoor air quality. Thus, all design team members must weigh this possibility and consider all potential loads for the concept design.
Technical factors
Technical factors in Vietnam’s medical system encompass five key variables, with “T4”, known for its compatibility with the medical system, “T2” operability, “T5” emissions level, “T3” integrated capability, and “T1” feasibility. The use of technological advancement is a critical concern in contemporary hospital construction to ensure adherence to intricate healthcare facility standards and facilitate the integration of medical equipment[40]. In the context of Vietnam, technology transfer and collaboration are vital. Forming partnerships with more developed nations or international organisations can be highly advantageous for Vietnam, involving not only acquiring the physical technology but also mastering the necessary skills and training for its effective operation and maintenance. Limitations in installing building service systems in Vietnam are related to the skills of the design and construction consultants, non-compliance with regulations and lack of inspection and evaluation. Therefore, it is crucial to foster local innovation and adaptation in Vietnam by consistently upgrading technology and enhancing the skills of companies. This involves developing solutions tailored explicitly to Vietnamese hospitals’ unique needs and resource limitations, such as employing low-cost materials or more straightforward, more maintainable technologies. Additionally, in Vietnam, prioritising low-cost technology, like basic air filters or mixed-mode combinations of natural ventilation methods, can serve as an initial step in enhancing air quality[9,39,46]. To maintain IAQ in use, management and maintenance activities, ventilation systems, cleaning and disinfection activities, and contaminant control plans are conducted by professionals in the facility[7,41,47]. Creating a database that tracks IAQ metrics, pollutant types, and quantities in various indoor environments may result in prompt response and legislative changes.
6. Conclusion
Healthcare facilities in Vietnam are at risk of infections and building-related syndromes due to inadequate indoor air. Although extensive technological solutions and research have been conducted worldwide on IAQ’s design, installation, and operation, they are scarce and restricted to individual perspectives in Vietnam. We reviewed existing literature on factors influencing construction technology adoption and architectural factors that affect the quality of indoor air in hospital projects. This study collects and analyses 160 surveyors to identify 16 priority factors relying on the selection of IAQ advances; we pave the way for more informed choices in adopting integrated technologies, fostering healthier indoor environments, and ensuring occupants’ health in healthcare buildings.
The median value and factor analysis are applied to reveal four main factors in selecting IAQ improvement solutions: Economic, Design, Governance, and Technical. Intergroup comparison test results show that stakeholders considering IAQ solutions often prioritise factors relevant to their specific areas of expertise. This inclination is partly attributable to the disparities among contractor companies and their distinct knowledge and proficiency in the field. Firstly, to promote effective collaboration, an integrated design team will proffer unified solutions according to the articulated needs of investors, market demands, and the prevailing legal framework. This overarching design concept serves as a guiding principle throughout IEQ-related design, commencing from the conceptual phase to occupancy. Secondly, knowledge and critical factors must be considered, from concept design to construction and operation, to maintain the IAQ and ensure healthcare activities are met. Medical employees, including nurses and facility staff, have expressed little understanding of ventilation’s efficacy in large-scale hospitals’ strenuous environments. Additionally, they frequently need to prioritise the quality of ventilation, poor air quality, noxious emissions from interior materials, and an excessive rise in humidity. Lastly, the utilisation of indoor sensors and monitors provides the IAQ index, educates and trains personnel to effectively manage spaces and operate ventilation systems, and enables them to recognise the early warning signs and impact on their health.
However, it is important to note that our research has limitations, including the sample size and geographical context. 65% of those surveyed abstained from engaging in healthcare projects and needed more comprehension of the unique prerequisites associated with healthcare. Only 5% of respondents from healthcare design companies demonstrated a comprehensive understanding of prevalent difficulties in this field and the most recent national legislation. We recommend further investigations to validate the applicability of these critical factors through in-depth case studies and assessments in different regions. It is imperative to recognise that developing a sustainable building requires careful consideration of local contextual factors and a thorough exploration of national standards pertaining to construction practices, particularly in densely urban areas within Vietnam. This will contribute to a more comprehensive understanding of IAQ improvement alternatives for healthcare projects across developing countries, providing insights that can inform future practices, certifications, and policies.
Supplementary materials
The supplementary material for this article is available at: Supplementary materials.
Authors contribution
All authors contributed equally to this work.
Conflicts of interest
All authors declare no conflicts of interest.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
The data and materials could be obtained from the corresponding author.
Funding
None.
Copyright
© The Author(s) 2024.
References
-
1. Mendes AS, Teixeira JP. Sick building syndrome. In: Wexler P, editor. Encyclopedia of Toxicology. New York: Elsevier Inc. Academic Press; 2014. p. 256-260.[DOI]
-
2. Hai ND, Thy LL, Chanh DN. Prevalence of sick building syndrome-related factors among hospital workers at University Medical Center Ho Chi Minh City, Vietnam. Med Pharm Res. 2018;2(2):1-4.[DOI]
-
3. Nguyen HTT, Nguyen GNT, Nguyen AV. Hospital-acquired infections in ageing Vietnamese population: current situation and solution. Med Pharm Res. 2020;4(2):1-10.[DOI]
-
4. Lee HJ, Lee KH, Kim DK. Evaluation and comparison of the indoor air quality in different areas of the hospital. Medicine. 2020;99(52):e23942.[DOI]
-
5. Keyvani S, Mohammadyan M, Chimehi E. Effect of the meteorological parameters on the indoor PM2.5 and PM10 concentrations in a hospital. SRPH J Med Sci Healthc Manag. 2020;2(4):1-7.[DOI]
-
6. Liu Y, Wang Z, Zhang Z, Hong J, Lin B. Investigation on the Indoor Environment Quality of health care facilities in China. Build Environ. 2018;141:273-287.[DOI]
-
7. Settimo G. Existing guidelines for indoor air quality: the case study of hospital environments. In: Capolongo S, Settimo G, Gola M, editors. Indoor Air Quality in Healthcare Facilities. Cham: Springer; 2017. p. 13-26.[DOI]
-
8. Farraia M, Paciência I, Ribeiro A I, Moreira A, Cavaleiro Rufo J. Indoor air quality in hospitals: How is the situation in Portugal? In: Arezes PM, Baptista JS, Barroso MP, Carneiro P, Cordeiro P, Costa N, Melo RB, Miguel S, Perestreloeditors G, editors. Occupational and Environmental Safety and Health. Studies in Systems, Decision and Control; 2022. p. 303-311.[DOI]
-
9. Lasomsri P, Yanbuaban P, Kerdpoca O, Ouypornkochagorn T. A development of low-cost devices for monitoring indoor air quality in a large-scale hospital. In: 2018 15th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON); 2018 Jul 18-21; Chiang Rai, Thailand. Piscataway: IEEE; 2018. p. 282-285.[DOI]
-
10. Nimlyat PS. Indoor environmental quality performance and occupants’ satisfaction [IEQPOS] as assessment criteria for green healthcare building rating. Build Environ. 2018;144:598-610.[DOI]
-
11. Wei W, Ramalho O, Mandin C. Indoor air quality requirements in green building certifications. Build Environ. 2015;92:10-19.[DOI]
-
12. ASHRAE [Internet]. Atlanta: The Association. Available from: https://www.ashrae.org
-
13. U.S. Green Building Council. LEED v4.1 Building Design and Construction [Internet]; 2023. Available from https://www.usgbc.org/leed/v41
-
14. Kim S, Osmond P. Analyzing green building rating tools for healthcare buildings from the building user’s perspective. Indoor Built Environ. 2013;23(5):757-766.[DOI]
-
15. Radha CH. Retrofitting for improving indoor air quality and energy efficiency in the hospital building. Sustainability. 2023;15(4):3464.[DOI]
-
16. Hiwar W, King MF, Shuweihdi F, Fletcher LA, Dancer SJ, Noakeset CJ. What is the relationship between indoor air quality parameters and airborne microorganisms in hospital environments? A systematic review and meta‐analysis. Indoor Air. 2021;31(5):1308-1322.[DOI]
-
17. Rodrigo MNN, Kosala Y, Perera B, Dalugoda C. Mitigation of hospital acquired infections in developing countries through the provision of a better IAQ. Eng J Inst Eng Sri Lanka. 2018;51(1):39-48.[DOI]
-
18. Ratajczak K. Ventilation strategy for proper IAQ in existing nurseries buildings-lesson learned from the research during COVID-19 pandemic. Aerosol Air Qual Res. 2022;22(3):210337.[DOI]
-
19. Stockwell RE, Ballard EL, O’Rourke P, Knibbs LD, Morawska L, Bell SC. Indoor hospital air and the impact of ventilation on bioaerosols: A systematic review. J Hosp Infect. 2019;103(2):175-184.[DOI]
-
20. Sloan Brittain O, Wood H, Kumar P. Prioritising indoor air quality in building design can mitigate future airborne viral outbreaks. Cities Health. 2021;5(sup1):S162-S165.[DOI]
-
21. Ikhtiar M, Alzad H, Paramita S, Yasir Y. Microbiological assessment of indoor air of takalar county hospital wards in south Dulawesi, Indonesia. Sci J Public Health. 2017;5(3):172-177.[DOI]
-
22. Olsson NEO, Hansen GK. Identification of critical factors affecting flexibility in hospital construction projects. HERD. 2010;3(2):30-47.[DOI]
-
23. American Society of Heating, Refrigerating and Air-Conditioning Engineers. Residential indoor air quality guide: best practices for acquisition, design, construction, maintenance and operation. Atlanta (GA): ASHRAE; 2018. Available from: https://www.ashrae.org/technical-resources/bookstore/indoor-air-quality-guide [DOI:10.1016/j.proeng.2015.08.538][DOI]
-
24. AlSanad S. Awareness, drivers, actions, and barriers of sustainable construction in Kuwait. Procedia Eng. 2015;118:969-983.[DOI]
-
25. Hussain K, He Z, Ahmad N, Iqbal M, Taskheer Mumtaz SM. Green, lean, six sigma barriers at a glance: A case from the construction sector of Pakistan. Build Environ. 2019;161:106225.[DOI]
-
26. Nguyen HT, Skitmore M, Gray M, Zhang X, Olanipekunt AO. Will green building development take off? An exploratory study of barriers to green building in Vietnam. Resour Conserv Recycl. 2017;127:8-20.[DOI]
-
27. Yang J, Yang Z. Critical factors affecting the implementation of sustainable housing in Australia. J Hous Built Environ. 2015;30(2):275-292.[DOI]
-
28. Afful AE, Ayarkwa J, Acquah GKK, Osei-Asibey D, Osei Assibey AAD. Barriers to incorporation of indoor environmental quality (IEQ) principles into building designs. Eng Constr Archit Manag. 2023;30(6):2400-2419.
-
29. Ahn YH, Pearce AR, Wang Y, Wang G. Drivers and barriers of sustainable design and construction: The perception of green building experience. Int J Sustainable Build Technol Urban Dev. 2013;4(1):35-45.[DOI]
-
30. Darko A, Zhang C, Chan APC. Drivers for green building: A review of empirical studies. Habitat Int. 2017;60:34-49.[DOI]
-
31. Plessis CD. A strategic framework for sustainable construction in developing countries. Constr Manage Econ. 2007;25(1):67-76.[DOI]
-
32. Leung M, Chan AHS. Control and management of hospital indoor air quality. Med Sci Monitor. 2006;12(3):SR17-SR23.[PubMed]
-
33. MacNaughton P, Pegues J, Satish U, Santanam S, Spengler J, Allen J. Economic, environmental and health implications of enhanced ventilation in office buildings. Int J Environ Res Public Health. 2015;12(11):14709-14722.[DOI]
-
34. Razali NM, Wah YB. Power comparisons of shapiro-wilk, kolmogorov-smirnov, lilliefors and anderson-darling tests. J Stat Model Anal. 2011,2(1):21-33. Available from: https://www.nrc.gov/docs/ml1714/ml17143a100.pdf
-
35. Fellows RF, Liu AMM, Research methods for construction. 5th ed. Hoboken: Wiley-Blackwell; 2021.
-
36. Han Y, Jin R, Wood H, Yang T. Investigation of demographic factors in construction employees’ safety perceptions. KSCE J Civ Eng. 2019;23:2815-2828.[DOI]
-
37. Pandey AK, Dixit S, Bansal S, Saproo S, Mandal SN. Optimize the infrastructure design of hospital construction projects to manage hassle free services. Int J Civ Eng Technol. 2017;8(10):87-98. Available from: https://iaeme.com/MasterAdmin/Journal_uploads/IJCIET/VOLUME_8_ISSUE_10/IJCIET_08_10_011.pdf
-
38. Gou Z, Lau SSY, Prasad D. Market readiness and policy implications for green buildings: Case study from hong kong. J Green Build. 2013;8(2):162-173.[DOI]
-
39. Zhang Y, Mo J, Li Y, Sundell J, Wargocki P, Zhang J, et al. Can commonly-used fan-driven air cleaning technologies improve indoor air quality? A literature review. Atmos Environ. 2011;45(26):4329-4343.[DOI]
-
40. Liu W, Chan APC, Chan MW, Darko A, Oppong GD. Key performance indicators for hospital planning and construction: a systematic review and meta-analysis. Eng Constr Archit Manag. 2024;31(5):2151-2175.[DOI]
-
41. Kim J, Hong T, Lee M, Jeong K. Analyzing the real-time indoor environmental quality factors considering the influence of the building occupants’ behaviors and the ventilation. Build Environ. 2019;156:99-109.[DOI]
-
42. Ibrahim F, Samsudin EZ, Ishak AR, Sathasivam J. Hospital indoor air quality and its relationships with building design, building operation, and occupant-related factors: A mini-review. Front Public Health. 2022;10:1067764.[DOI]
-
43. Mittal YK, Paul VK, Rostami A, Riley M, Sawhney A. Delay factors in construction of healthcare infrastructure projects: a comparison amongst developing countries. Asian J Civ Eng. 2020;21:649-661.
-
44. Wang W, Pasquire S, Pasquire C. Factors for the adoption of green building specifications in China. Int J Build Pathol Adapt. 2018;36(3):254-267.[DOI]
-
45. Agyekum K, Adinyira E, Ampratwum G. Factors driving the adoption of green certification of buildings in Ghana. Smart Sustain Built Environ. 2020;9(4):595-613.[DOI]
-
46. Jung CC, Wu PC, Tseng CH, Su HYPERLINK "https://scholar.google.com/citations?user=uv6_au4AAAAJ&hl=zh-CN&oi=sra" HJ. Indoor air quality varies with ventilation types and working areas in hospitals. Build Environ. 2015;85:190-195.[DOI]
-
47. Clausen G. Ventilation filters and indoor air quality: a review of research from the International Centre for Indoor Environment and Energy. Indoor Air. 2004;14:202-207.[DOI]
Copyright
© The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Publisher’s Note
Science Exploration remains a neutral stance on jurisdictional claims in published
maps
and institutional affiliations. The views expressed in this article are solely those
of
the author(s) and do not reflect the opinions of the Editors or the publisher.
Share And Cite



Science Exploration Style
Anh DNH, Han AY, Thao TN, Binyumen MSA, Hoang PD. A comprehensive analysis of factors influencing the selection of indoor air quality improvement solutions for healthcare projects in Vietnam. J Build Des Environ. 2024;2:28343. https://doi.org/10.37155/2811-0730-0302-10
Tips
Copy completed.
Submit a Manuscript
Author Instructions
Cite this Article
Article Metrics
0
View
0
Download
Cited
Article Updates

- Abstract
- Keywords
- 1. Introduction
- 2. Literature Review
- 3. Research Methods
- 4. Results
- 5. Discussion
- 6. Conclusion
- Supplementary materials
- Authors contribution
- Conflicts of interest
- Ethical approval
- Consent to participate
- Consent for publication
- Availability of data and materials
- Funding
- References
- Copyright
Science Exploration Style
Anh DNH, Han AY, Thao TN, Binyumen MSA, Hoang PD. A comprehensive analysis of factors influencing the selection of indoor air quality improvement solutions for healthcare projects in Vietnam. J Build Des Environ. 2024;2:28343. https://doi.org/10.37155/2811-0730-0302-10
copy
Share Link
copy