AI-ECG for wearable monitoring: From arrhythmia diagnosis to early warning and multi-disease prediction
Zhiyuan Li
1,2,*

,
Yuanyuan Tian
1,2
,
Yanrui Jin
1,2
,
Chengliang Liu
1,2
*Correspondence to:
Zhiyuan Li, State Key Laboratory of Mechanical System and Vibration, School of Mechanical Engineering, Shanghai Jiao Tong University, Shanghai 200240, China.
E-mail: lzy2030@sjtu.edu.cn
BME Horiz. 2026;4:202619. 10.70401/bmeh.2026.0029
Received: April 01, 2026Accepted: June 08, 2026Published: June 08, 2026
Abstract
Wearable electrocardiography (ECG) is shifting cardiovascular monitoring from episodic in-hospital testing to continuous out-of-hospital assessment. Artificial intelligence-enabled ECG (AI-ECG) provides a new pathway for extracting clinically useful information from out-of-hospital wearable recordings. This review is organized around the wearable AI-ECG monitoring pipeline, summarizing key advances in model development, clinical application, and real-world validation, while emphasizing the special requirements that wearable scenarios impose on algorithm design and clinical translation. At present, arrhythmia screening remains the most mature application of AI-ECG, with deep learning models achieving cardiologist-level or clinician-comparable performance in several well-defined tasks. With the growing availability of long-term continuous recordings, research is further extending from post-event recognition to pre-event warning, particularly for high-risk events such as acute atrial fibrillation and malignant ventricular arrhythmias. Related methods are evolving from traditional feature-based machine learning toward deep learning and foundation models that can exploit waveform morphology, rhythm dynamics, and long-range temporal information. Beyond rhythm disorders, AI-ECG is also being explored for structural cardiac abnormalities, metabolic disorders, and broader systemic risk prediction, suggesting a potential role for ECG as a digital biomarker platform. However, several barriers continue to limit clinical translation, including limited cross-device and cross-population generalizability, insufficient interpretability, and the lack of prospective real-world validation. Future progress will likely depend on standardized data systems, artifact-aware modeling, cross-device validation, foundation models, longitudinal risk modeling, and intelligent systems designed for clinical workflows. Overall, wearable AI-ECG is evolving from passive abnormality detection toward continuous, proactive, and personalized health risk assessment.
Keywords
Wearable ECG monitoring, artificial intelligence-enabled ECG, arrhythmia diagnosis, early warning, deep learning
1. Introduction
Cardiovascular disease (CVD) remains one of the leading causes of death and disability worldwide, posing a substantial public health burden[1,2]. Among its major manifestations, arrhythmias are particularly challenging because they often have silent onset, intermittent occurrence, and potentially rapid clinical deterioration, making continuous monitoring critical for timely detection and intervention[3]. Although conventional 12-lead electrocardiography (ECG) and Holter monitoring are fundamental tools for cardiac assessment, their utility is limited by short monitoring duration, restricted portability, dependence on expert interpretation, and limited suitability for long-term out-of-hospital management[4]. With the advent of smartwatches and ECG patches, wearable ECG monitoring has become an important approach for continuous CVD management[5,6].
Recent advances in artificial intelligence, particularly artificial intelligence-enabled ECG (AI-ECG), are reshaping the conventional use of ECG[7]. Driven by deep learning, AI-ECG not only improves the accuracy of arrhythmia diagnosis but also shows promise for early warning of high-risk cardiac events and risk assessment across multiple noncardiac systems[8]. In wearable settings, these capabilities are transforming ECG from a signal-recording tool into a platform for continuous health sensing and risk prediction, creating new opportunities for out-of-hospital monitoring, chronic disease management, and personalized intervention[8]. In this setting, model performance is tightly coupled to single- or few-lead acquisition, motion artifacts, electrode contact, sampling differences, and longitudinal individual variability, which makes wearable AI-ECG a distinct real-world modeling problem rather than a direct extension of hospital-based ECG analysis[9].
As summarized in Figure 1, wearable AI-ECG monitoring can be organized as a workflow that begins with wearable ECG sensors, proceeds through data acquisition and mobile/cloud transmission, and then connects AI analysis with clinical tasks and output feedback. Wearable AI-ECG can support a closed-loop management framework in which ECG signals are acquired by wearable devices, transmitted to mobile or cloud-based systems, analyzed by AI algorithms, and returned to users or clinicians as risk estimates, alerts, or follow-up information. This human-in-the-loop workflow may improve long-term monitoring, triage, and individualized management, but also raises higher requirements for signal quality control, model reliability, and clinically actionable outputs.
{kind=link}
Figure 1. Workflow of AI-assisted wearable ECG monitoring. The figure summarizes data acquisition, mobile or cloud platform, AI analysis, clinical tasks, and user or clinician feedback. ECG: electrocardiography; AI: artificial intelligence.
Unlike previous AI-ECG reviews that mainly focus on diagnostic algorithms or cardiovascular applications, this review emphasizes wearable monitoring, where device constraints, model design, clinical tasks, and validation requirements are tightly coupled. As wearable AI-ECG continues to evolve, its scope is extending from arrhythmia diagnosis to more predictive and integrative applications, including early warning of impending arrhythmic events and disease prediction beyond rhythm disorders. These developments make it valuable to review wearable AI-ECG within a unified framework that connects signal characteristics, analytical pipelines, and downstream clinical tasks. In this framework, arrhythmia diagnosis, arrhythmia early warning, and selected cross-system risk prediction represent a progression from event detection to longitudinal health assessment.
Against this background, this review focuses on the development of AI-ECG in wearable monitoring, from arrhythmia diagnosis to arrhythmia early warning and multi-disease prediction. We first summarize wearable ECG devices, data-collection workflow, signal characteristics, and the general analytical pipeline of wearable AI-ECG. We then review recent progress in three major application domains: arrhythmia diagnosis, early warning of impending arrhythmic events, and broader disease prediction beyond rhythm disorders. Here, multi-disease prediction refers to selected ECG-based assessments of cardiac structural and functional abnormalities, metabolic or electrolyte disorders, physiological aging and prognosis, and systemic risk indicators. Finally, we discuss the key barriers to clinical translation, including data limitations, generalizability, interpretability, and real-world deployment, and outline future directions for wearable AI-ECG research and practice. Particular attention is given to standardized datasets, cross-device and cross-population validation, prospective evaluation, foundation models, longitudinal risk modeling, and different reliability requirements for wellness monitoring and clinical decision support.
2. Overview of AI-ECG for Wearable Monitoring
2.1 Wearable ECG devices and data-collection workflow
ECG records cardiac electrical activity through body-surface electrodes, and conventional 12-lead ECG remains the clinical standard for evaluating rhythm disorders, conduction abnormalities, ischemia, and related cardiac conditions, as shown in Figure 2a. Wearable ECG monitoring is shifting ECG assessment from short-term in-hospital testing to continuous out-of-hospital monitoring. Wearable devices, including Holter monitors, ECG patches, smartwatches, chest straps, and flexible electronic systems[10], emphasize portability, wearing comfort, and remote transmission, thereby changing ECG from a one-time clinical recording into a continuous real-world data source for AI-driven analysis[11-13].
{kind=link}
Figure 2. Clinical and wearable ECG acquisition. (a) Standard multi-lead clinical ECG; (b) Wearable ECG, where electrode contact, body motion, and device settings affect signal quality and AI analysis. ECG: electrocardiography; AI: artificial intelligence; BW: baseline Wander; EM: electrode motion; MA: motion artifact.
For AI development, the usefulness of wearable ECG data depends not only on recording volume but also on the acquisition workflow. Key factors include electrode position, skin-electrode contact, device fixation, sampling rate, filtering settings, recording duration, recording context, and symptom or activity logs. Because annotations may come from expert review, device-generated events, clinical reports, symptom-triggered recordings, or linked outcomes, wearable ECG datasets should clearly report device type, lead configuration, acquisition settings, population characteristics, labeling procedure, and signal-quality criteria.
2.2 Characteristics and key challenges of wearable ECG signals
Compared with standard clinical ECG, wearable ECG is characterized by limited lead information, stronger noise contamination, and greater temporal and inter-individual variability[14,15]. Most wearable devices acquire single-lead or few-lead signals, which provide less spatial information than 12-lead ECG and therefore constrain some diagnostic tasks[16,17]. In addition, wearable monitoring is performed in uncontrolled environments and is therefore highly vulnerable to multiple sources of signal contamination, as illustrated in Figure 2b, including baseline wander, motion artifacts, electromyographic interference, and other noise sources that may distort waveform morphology and compromise beat detection and interval measurement[18-20]. As long-term recordings also reflect diverse physiological states and marked individual heterogeneity, wearable ECG analysis is fundamentally a real-world modeling problem involving noisy, dynamic, and heterogeneous signals.
The main wearable-specific constraints and their modeling implications are summarized in Table 1 below. This mapping provides the technical basis for later discussions of arrhythmia diagnosis, early warning, and cross-system risk prediction.
Table 1. Wearable ECG constraints and their implications for modeling and validation.
| Wearable constraint | Effect on ECG analysis | Modeling and validation implication |
| single- or few-lead acquisition | Reduced spatial information and weaker visibility of some morphology patterns | Task-aware lead selection[21], lead-aware representation learning[22], cautious transfer from 12-lead ECG, and external validation[23] |
| Motion artifacts and baseline drift | Distorted morphology, unreliable R peaks or intervals, and false alarms | Signal quality assessment[24], denoising[25], and robust training[26] |
| Unstable electrode contact or dropout | Amplitude shifts, missing segments, and discontinuous long-term records | Segment-level quality flags, missing-data handling, temporal aggregation, and rejection rules for unusable intervals[27-29] |
| Sampling, filtering, and device differences | Device-dependent waveform detail and feature distributions | Transparent acquisition reporting, preprocessing harmonization, domain adaptation, and cross-device testing[30,31] |
| Individual and longitudinal variability | Different personal baselines and context-dependent rhythm or morphology changes | Subject-level splits[32,33], personalization[34], longitudinal modeling, calibration, and population-level validation[35] |
ECG: electrocardiography.
Common wearable artifacts include baseline wander related to respiration or posture change, electrode-motion artifacts caused by unstable skin-electrode contact, and muscle artifacts generated by skeletal muscle activity. Because these components may overlap with ECG waveforms in both time and frequency domains, they can distort P wave-QRS complex-T wave (P-QRS-T) morphology, interfere with R-peak detection and interval measurement, and increase false-positive or false-negative AI outputs.
2.3 General analytical pipeline of wearable AI-ECG
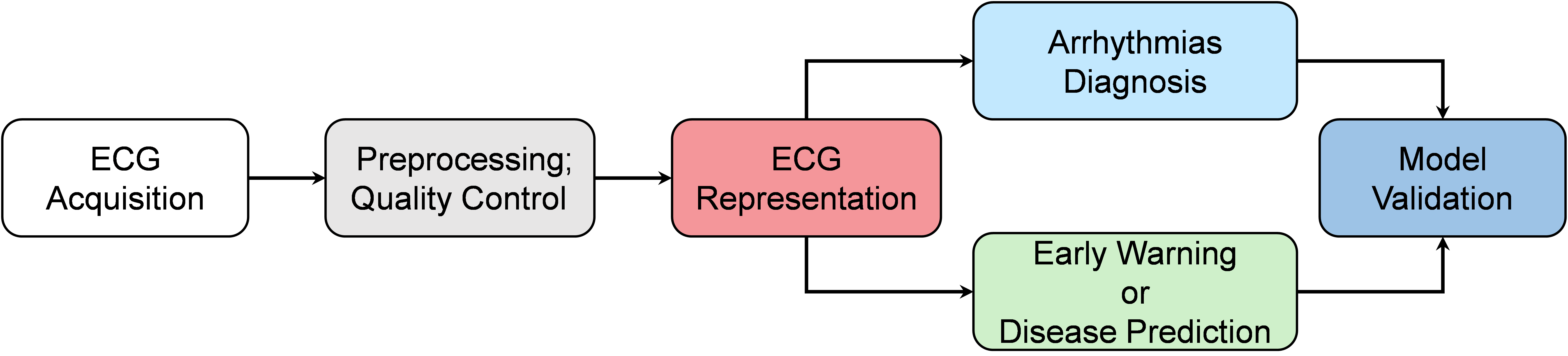
As shown in Figure 3, wearable AI-ECG generally involves signal acquisition, preprocessing and quality control, feature representation learning, downstream task modeling, and risk output. After ECG representation, the pipeline separates into two major application branches that correspond to the structure of this review: arrhythmia diagnosis, discussed in Section 3, and arrhythmia early warning or broader disease prediction, discussed in Section 4. This organization links wearable signal constraints to model design and then to clinically different evaluation requirements.
{kind=link}
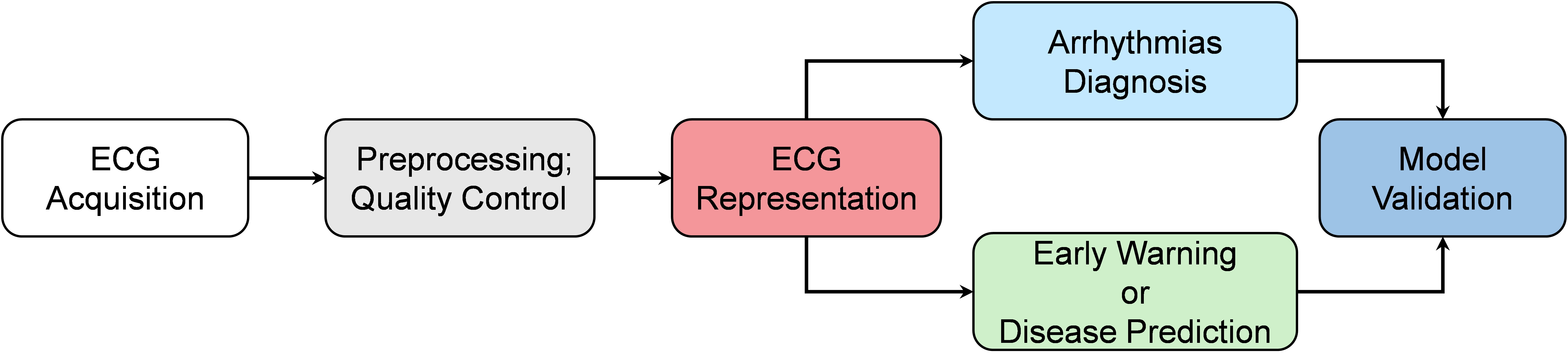
Figure 3. Analytical pipeline of wearable AI-ECG. ECG acquisition and quality control lead to ECG representation, task-specific modeling, and validation for diagnosis, early warning, or disease prediction. ECG: electrocardiography; AI-ECG: artificial intelligence-enabled ECG.
Preprocessing and quality control aim to make wearable signals usable under noisy conditions. Artifact-reduction approaches include conventional filtering and adaptive filtering[19], wavelet or empirical-mode decomposition[36], nonlocal-means and related signal-processing methods[37], deep denoising models such as denoising autoencoders[38], convolutional neural network (CNN)/recurrent neural network (RNN)-based networks[39], generative adversarial network-based methods[40], and diffusion-based models[41]. Beyond denoising, artifact-aware AI systems may use noise augmentation, signal-quality gating, robust loss functions, missing-segment handling, and uncertainty estimation to reduce unsafe predictions from low-quality segments.
Modeling strategies can be organized by input representation. Feature-based models[42-46] use extracted physiological parameters, including R-R intervals, heart rate variability (HRV), ECG intervals, waveform morphology, ST-T features, ectopic burden, frequency-domain HRV, and nonlinear indices, followed by conventional machine learning or shallow neural networks. These methods are interpretable and data-efficient but depend strongly on signal quality and accurate fiducial-point detection. Full-signal deep learning models instead learn from raw or minimally processed ECG segments. CNNs[47] capture local waveform and beat-level morphology, RNNs and long short-term memory (LSTMs)[16] model rhythm dynamics, and Transformer-based[22], self-supervised[48], or foundation-model[49,50] approaches may improve long-range representation learning and transferability.
After representation learning, model objectives should be defined by the downstream clinical task. Arrhythmia diagnosis mainly requires reliable identification of rhythm events or heartbeat categories from noisy long-term recordings. In contrast, arrhythmia early warning and disease prediction require models to capture pre-event, longitudinal, or latent physiological patterns rather than only overt abnormalities. Across these branches, validation should include patient-level data separation, external and cross-device testing, calibration, and clinically interpretable outputs; a more detailed staged validation framework is discussed in Section 5.
3. AI-ECG for Arrhythmia Diagnosis
3.1 Clinical need for arrhythmia diagnosis in wearable settings
Arrhythmia diagnosis is the most direct and currently the most mature application of wearable AI-ECG. Its main value lies in overcoming the limited ability of static ECG and short-term monitoring to capture paroxysmal abnormalities. This is particularly important for conditions such as atrial fibrillation, premature atrial or ventricular contractions, and intermittent atrioventricular block, which are often brief or clinically subtle and therefore prone to missed diagnosis during routine short-duration ECG assessment[51-53]. Among these applications, AF screening is the most representative because of its high prevalence, major association with stroke and heart failure, and strong suitability for long-term wearable monitoring. Large-scale studies such as the Apple Heart Study and related wearable AI investigations have demonstrated the feasibility of AF screening in both general and high-risk populations[54].
Compared with many structural or ischemic ECG tasks, arrhythmia analysis is particularly compatible with wearable ECG because rhythm disorders are often expressed through temporal patterns, R-R irregularity, ectopic burden, and beat morphology, which can be captured by single- or few-lead long-term recordings. However, the clinical meaning of arrhythmia outputs differs across use cases. Consumer-facing screening mainly aims to identify possible abnormal rhythms for follow-up, whereas clinical decision support requires higher reliability, lower false-alarm burden, and clearer evidence for actionable intervention.
3.2 Main methods for arrhythmia diagnosis
Arrhythmia models can be broadly divided into feature-based and full-signal approaches. Feature-based methods use fiducial points and physiological parameters such as RR intervals, HRV, PR/QRS/QT measures, P-wave or QRS morphology, ST-T patterns, ectopic burden, and nonlinear rhythm indices, followed by rule-based classifiers, support vector machines (SVMs), random forests, gradient boosting, logistic regression, or shallow neural networks[44-46]. These methods are interpretable and data-efficient, but their performance may degrade when wearable noise, poor electrode contact, or motion artifacts impair fiducial-point detection.
Full-signal deep learning models learn diagnostic representations directly from raw or minimally processed ECG and have achieved strong performance in ambulatory single-lead and large clinical 12-lead benchmarks[16,17,52,54-56]. CNNs are commonly used to capture local waveform and beat-level morphology, RNNs or LSTMs model sequential rhythm dynamics, and Transformer or pretrained representation models may improve long-range context modeling and transferability. Representative studies are summarized in Table 2.
Table 2. Representative studies for arrhythmias diagnosis.
| Year | Study | Dataset | Task | Performance | Model | Wearable relevance or limitation |
| 2019 | Hannun et al.[16] | 91,232 (single-lead) | 12 rhythm classes | AUC:0.97F1:0.837 | CNN | Strong evidence for single-lead ambulatory arrhythmia classification, but performance depends on recording quality and annotation consistency |
| 2020 | Zhu et al.[56] | 180,112 (12-lead) | 21 rhythm/conduction labels | F1:0.845 | CNN | Demonstrates multilabel AI-ECG diagnosis, but transfer to wearable few-lead signals requires separate validation |
| 2020 | Ribeiro et al.[57] | 2,322,513 (12-lead) | 6 arrhythmia classes | F1:0.8 | CNN | Large-scale clinical benchmark; not directly equivalent to noisy wearable single-lead deployment |
| 2022 | Sangha et al.[58] | 2,228,236 (12-lead) | Arrhythmia or ECG abnormality | AUC:0.99 | EfficientNet-B3 | Shows scalability of image/deep learning approaches, but device and lead differences remain important |
| 2024 | Jin et al.[17] | 352,725 (single-lead) | 6 arrhythmia classes | F1:0.83AUC:0.977 | ResNet + LSTM | More directly relevant to wearable single-lead diagnosis and illustrates the value of temporal modeling and interpretability |
CNN: convolutional neural network; ECG: electrocardiography; AI-ECG: artificial intelligence-enabled ECG; LSTM: long short-term memory; AUC: area under the receiver operating characteristic curve.
Together, these studies show that arrhythmia diagnosis is the most mature application of wearable AI-ECG. However, Table 2 also highlights a translational distinction: strong retrospective performance should be interpreted together with lead configuration, device type, annotation quality, and validation setting, especially when models are transferred from standard 12-lead ECG to noisier single- or few-lead wearable recordings.
3.3 Current challenges
Despite its expert-level performance, AI-ECG for arrhythmia diagnosis still faces several important limitations. Deep learning models’ performance often declines across devices, lead configurations, sampling settings, and patient populations, indicating limited generalizability[23,30]. In real-world monitoring, noise, motion artifacts, and low-quality segments remain major sources of false positives and false negatives. More complex tasks, including fine-grained classification of supraventricular and ventricular arrhythmias, multilabel recognition, and rare-event detection in long recordings, also remain challenging because of class imbalance and annotation burden[56]. In addition, although deep models frequently outperform conventional methods, limited interpretability continues to hinder clinical trust[59-61].
For wearable deployment, these limitations should be translated into task-specific evaluation requirements. Beyond accuracy or area under the receiver operating characteristic curve (AUC), wearable arrhythmia systems should report signal-quality handling, patient-level validation, external and cross-device testing, false alarms per monitoring time, calibration, and clinician-interpretable evidence according to the intended use. These diagnostic challenges also define the boundary of event recognition: most current systems identify arrhythmias during or after their occurrence, whereas continuous wearable monitoring creates the opportunity to model pre-event risk states and broader longitudinal health signals, which motivates the frontier applications discussed in the next section.
4. Frontier Extensions of AI-ECG in Wearable Monitoring
4.1 Risk prediction: Expanding the capability boundary of AI-ECG
Whereas arrhythmia diagnosis focuses on detecting abnormalities after they occur, recent AI-ECG research has increasingly shifted toward risk prediction. Building on the diagnostic foundation discussed in Section 3, this shift asks whether long-term wearable ECG can reveal pre-event or latent physiological patterns before overt clinical abnormalities are recognized. Two directions have emerged: early warning of impending arrhythmic events and prediction of disease beyond rhythm disorders. Together, these developments mark a transition in wearable AI-ECG from passive detection to proactive risk assessment.
This shift reflects more than an expansion of task categories. It also indicates a change in analytical focus, from segment-level classification to longitudinal modeling, from overt waveform abnormalities to latent risk representations, and from single-disease detection to broader digital biomarker discovery[62]. Because wearable devices support continuous monitoring in real-world settings, they are particularly well suited for these emerging applications. Accordingly, this section discusses two frontier directions: arrhythmia early warning, which aims to identify pre-event risk states, and selected cross-system prediction, which explores ECG-derived digital biomarkers beyond rhythm diagnosis.
4.2 AI-ECG for arrhythmia early warning
Arrhythmia early warning is based on the assumption that clinically overt arrhythmia may be preceded by a transitional pre-event state rather than occurring instantaneously. Early studies of paroxysmal atrial fibrillation (PAF) suggested that ECG may contain detectable prodromal information before onset[63-65]. As shown in Figure 4, this transition may involve progressive or fluctuating changes in rhythm organization, ectopic activity, conduction, repolarization, and autonomic regulation.
{kind=link}
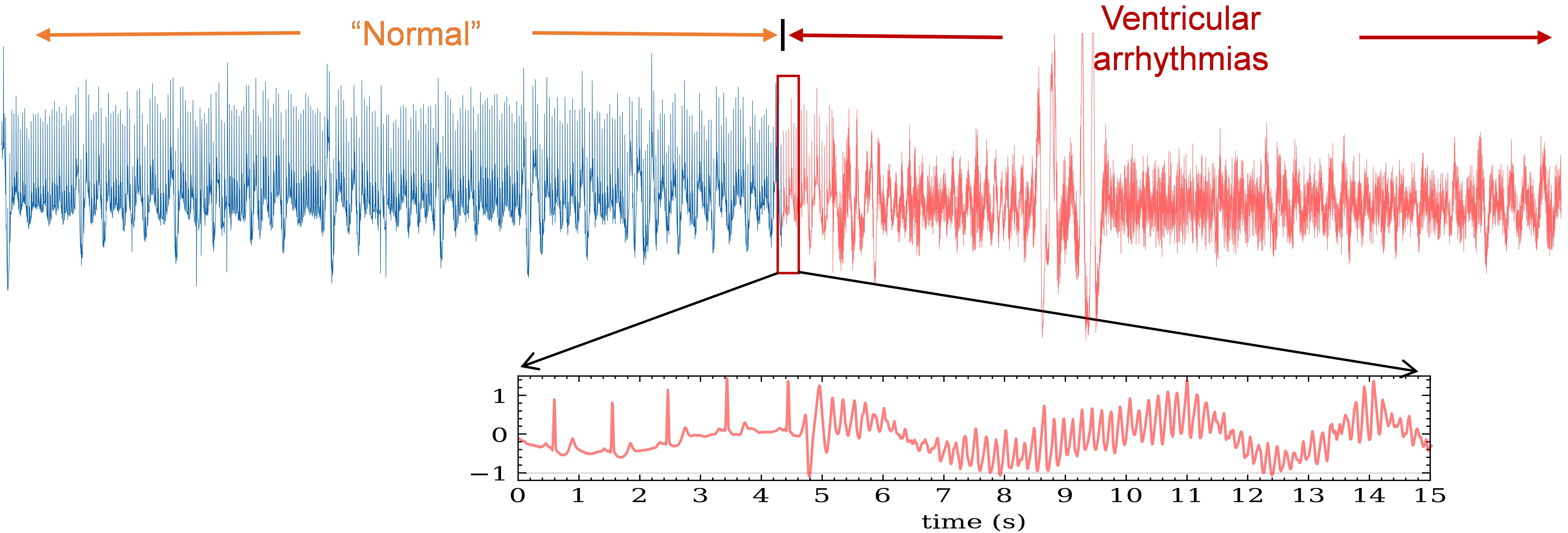
Figure 4. Pre-event evolution before arrhythmia onset. A conceptual transition from stable rhythm to arrhythmia may involve subtle changes in rhythm, ectopy, conduction, repolarization, and autonomic modulation.
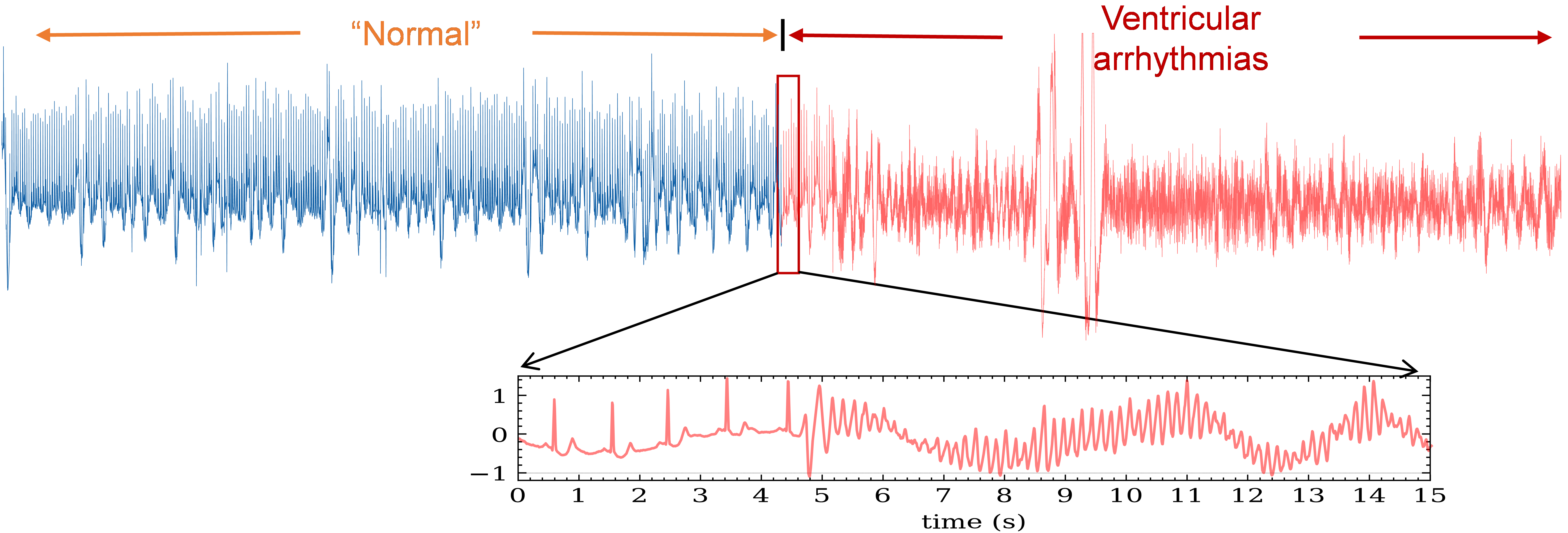
Long-term wearable ECG is therefore suited to early warning because weak and nonlinear pre-event patterns are difficult to identify by visual inspection but may be captured through continuous monitoring and AI-based modeling (Figure 5). In practice, an early-warning model must define the target event, observation window, pre-event window, prediction horizon, baseline or control window, and acceptable false-alarm burden[66], because these definitions directly affect training, reported performance, and clinical usefulness.
{kind=link}
Figure 5. Long-term ECG changes before malignant rhythm onset. Weak and nonstationary pre-event patterns may require continuous monitoring and AI-based analysis for detection. ECG: electrocardiography; AI: artificial intelligence.
For PAF, ventricular tachycardia, ventricular fibrillation, and related events, early-warning studies therefore aim to identify pre-event ECG changes before post-onset diagnosis is too late to guide timely intervention.
Existing methods can be divided into two broad groups. Feature-based studies usually extract R-R interval dynamics[67], ectopic activity[68], QT or repolarization indices[69], morphology descriptors[70], frequency-domain features[71], or nonlinear dynamics[72], and then use SVM, k-nearest neighbor, decision trees, XGBoost, Markov models, or related classifiers. These approaches are interpretable and data-efficient, but they depend on accurate beat detection and are sensitive to wearable noise and window definition. Full-signal or sequence-based approaches use CNNs, RNN/LSTMs, transfer learning, or self-supervised representations to learn warning patterns from raw or long-term ECG. These models may better capture nonlinear and long-range dependencies, but they require larger event datasets and careful prospective validation.
Table 3 summarizes representative patterns across early-warning studies rather than listing all reports individually. The key message is that prediction windows, feature sets, model families, and validation strategies vary substantially, making direct comparison difficult.
Table 3. Summary of representative arrhythmia early-warning studies.
| Task | Input features | Pre-event window | models | Main limitation |
| PAF onset detection | HRV, P-wave or ECG morphology | minutes before onset | SVM[67], KNN[63], Markov models[73], CNN[65] | Small datasets, inconsistent windows, and dependence on beat detection |
| PAF longer-horizon warning | HRV, rhythm type | From tens of minutes to several hours | XGBoost[13], CNN[74], | Limited evidence for cross-subject and cross-device generalization |
| VT/VF onset detection | HRV, repolarization, morphology, nonlinear dynamics, EMD or phase-space features | Seconds to tens of minutes before event | SVM[75], decision trees[76], KNN[77], transfer learning[78], hybrid models[79] | Rare events, heterogeneous endpoints, and high false-alarm cost |
| Long-term ambulatory deep warning | Raw ECG, long-term rhythm-morphology patterns, learned representations | Variable (based on duration before event onset) | CNN[80], LSTM[81] | Need prospective validation, calibration, and clinically meaningful alert thresholds |
PAF: paroxysmal atrial fibrillation; HRV: heart rate variability; ECG: electrocardiography; SVM: support vector machine; KNN: k-nearest neighbor; CNN: convolutional neural network; VT: ventricular tachycardia; VF: ventricular fibrillation; EMD: empirical mode decomposition; LSTM: long short-term memory.
Recent deep learning studies have begun to revisit this problem by learning latent warning patterns directly from long-term ECG recordings. As shown in Figure 6a, using recordings longer than 20 hours, Fiorina et al.[82] and Gavidia et al.[83] applied convolutional neural networks to pre-event ECG and demonstrated the potential of deep models to identify prodromal signatures before arrhythmias. Related work further suggests that these warning patterns are nonlinear, exhibit long-term dependency, and jointly involve rhythm and morphological changes[81], shown in Figure 6b. Nevertheless, this field remains less mature than arrhythmia diagnosis because of limited event samples, inconsistent pre-event definitions, inter-individual variability, motion-related false alarms, uncertain clinical actionability, and lack of prospective real-world testing.
{kind=link}
Figure 6. Long-term ECG modeling for arrhythmia early warning. (a) Pre-event ECG can be used to estimate near-term arrhythmia risk; (b) Deep sequence models can learn nonlinear rhythm-morphology changes. ECG: electrocardiography; CNN: convolutional neural network; LSTM: long short-term memory.
4.3 AI-ECG for multi-disease prediction and cross-system health assessment
Another extension of AI-ECG is the prediction of selected diseases beyond rhythm abnormalities. Because ECG reflects conduction, repolarization, structural remodeling, autonomic regulation, metabolic status, and electrolyte balance, AI methods may uncover latent physiological information not readily accessible through visual interpretation. Recent AI-ECG digital biomarker platforms further reflect this shift from single-task diagnosis toward systematic ECG-derived phenotype exploration. Here, multi-disease prediction refers to selected ECG-based assessments of cardiac structural or functional abnormalities, metabolic and electrolyte disturbances, physiological aging or prognosis, and systemic risk indicators, rather than unrestricted diagnosis of all diseases.
Current studies include reduced left ventricular ejection fraction[62], heart failure risk[84], myocardial hypertrophy[85], and ischemia-related states[86-88]. These tasks are clinically attractive, but much of the supporting evidence still relies on standard clinical ECG rather than wearable single- or few-lead signals.
AI-ECG has also been explored for cross-system tasks, including hyperkalemia[89], physiological age estimation[90], and prediction of hospitalization or mortality risk[35]. Some studies further use explainability methods to relate model outputs to candidate waveform or frequency-domain patterns. As summarized in Figure 7, these studies suggest that AI-ECG may serve as a digital biomarker platform, but the evidence strength differs markedly across tasks. Recent wearable digital medicine studies combining ECG with other biosignals, such as PPG, also indicate broader interest in physiological state assessment, although such multimodal applications require separate validation and are not the main focus of this ECG-centered review.
{kind=link}
Figure 7. AI-ECG for cross-system prediction and interpretation. (a) AI-ECG may identify selected cardiac, metabolic, prognostic, and systemic risk signals; (b) Explainability methods can localize candidate ECG patterns but remain hypothesis-generating. ECG: electrocardiography; AI-ECG: artificial intelligence-enabled ECG.
However, this field remains less mature than arrhythmia diagnosis. Labels often rely on imaging, laboratory tests, follow-up data, or clinical endpoints, and it remains uncertain whether wearable single- or few-lead signals are sufficient for stable cross-disease prediction. These indirect physiological pathways also make interpretation and appropriate clinical use more challenging.
For wearable translation, cross-system AI-ECG should therefore be evaluated with stricter attention to label quality, lead configuration, external validation, calibration, and clinical actionability. These requirements are especially important because many cross-disease predictions depend on indirect ECG patterns rather than visually obvious diagnostic signs.
5. Challenges and Future Perspectives
5.1 Challenges
Despite the rapid expansion of AI-ECG in wearable monitoring, several challenges still limit its clinical translation.
First, data availability and annotation remain major bottlenecks. Although wearable devices can generate large volumes of continuous ECG data, high-quality datasets with standardized acquisition protocols and reliable clinical labels are still limited. This problem is especially pronounced in arrhythmia early warning and multi-disease prediction, where event samples are sparse, pre-event definitions are inconsistent, and labels often depend on additional examinations or long-term follow-up. For wearable ECG, dataset quality depends not only on sample size but also on lead configuration, sampling rate, electrode placement, recording context, signal-quality criteria, annotation source, and patient-level metadata. Without these details, model performance is difficult to compare or reproduce across studies.
Second, model generalizability remains insufficient. Wearable ECG data vary substantially across devices, lead configurations, sampling frequencies, wearing positions, and use scenarios. Patient populations also differ in age, comorbidity burden, and physiological status. Such heterogeneity can lead to marked performance degradation when models are transferred across datasets or deployed in practice. In addition, motion artifacts, noise, and low-quality segments remain common in wearable recordings and continue to challenge model stability. These factors make cross-device and cross-population generalization a central barrier for wearable AI-ECG.
Third, interpretability and clinical trustworthiness remain unresolved. Although deep learning models often outperform conventional methods, their decision logic is still not sufficiently transparent[60,91]. In wearable monitoring, where outputs may influence long-term management and clinical decision-making, accuracy alone is not enough. This concern is even more critical in early warning and multi-disease prediction, where the underlying mechanisms are less direct and the consequences of uncertainty may be greater. Clinically useful explanations should therefore link model outputs to interpretable ECG evidence, signal quality, temporal context, and uncertainty, rather than relying only on post-hoc heatmaps.
Finally, real-world validation and deployment remain limited. Many current studies are still based on retrospective datasets or offline analyses and have not been tested in long-term, real-world monitoring workflows. This limitation is particularly relevant to ECG denoising and artifact-reduction studies, which are often evaluated by signal-level metrics rather than downstream clinical utility. Important translational issues include false-alarm burden, handling of low-quality segments, clinician review workload, privacy protection, regulatory approval, continual model updating, and integration with wearable hardware and clinical workflows.
5.2 Future perspectives
Looking ahead, progress in wearable AI-ECG will depend not only on better algorithms, but also on advances in data infrastructure, validation, robustness, personalized risk assessment, and clinically usable intelligent systems. The most actionable priorities are standardized wearable ECG datasets, unified validation frameworks, artifact- and uncertainty-aware modeling, foundation and longitudinal ECG models, and clinical workflow integration.
First, large-scale, multicenter, multi-device real-world datasets will be essential for improving model generalizability and enabling prospective validation. This is particularly important for early warning and multi-disease prediction, where event samples are sparse and labels may depend on follow-up, imaging, or laboratory tests. A practical dataset protocol should report device type, lead placement, sampling frequency, filtering, recording context, signal-quality rules, annotation workflow, outcome linkage, and patient-level train-test separation.
Second, validation should move from internal testing with patient-level separation to external, cross-device, cross-lead, subgroup, and prospective real-world evaluation. In wearable monitoring, reliability should be judged not only by sensitivity, specificity, AUC, and calibration, but also by false alarms per monitoring time, handling of low-quality segments, clinician review burden, and clinical actionability.
Third, future models should treat signal quality and uncertainty as part of the inference process rather than as only preprocessing issues. Signal-quality assessment, artifact-aware training, quality-gated prediction, calibration, and uncertainty output may reduce false alarms and prevent overconfident predictions from low-quality wearable segments.
Fourth, foundation and longitudinal ECG models may support more scalable and personalized wearable AI-ECG. Self-supervised pretraining, masked autoencoders, and ECG foundation models can reduce reliance on task-specific labels and improve transferable representation learning, while longitudinal modeling may help distinguish stable individual baselines from clinically meaningful temporal changes. These models should still be evaluated for cross-device transfer, calibration, failure modes, subgroup performance, and interpretability before clinical use, especially when transferred from standard 12-lead ECG to wearable single- or few-lead recordings.
Finally, clinical workflow integration will determine whether wearable AI-ECG outputs can be translated into actionable care. Deployment should define alert thresholds, escalation rules, explanation formats, privacy safeguards, and clinician review pathways. LLM-based agents may help summarize ECG findings and support interactive decision-making[92], but their outputs should remain auditable and should support, rather than replace, clinician judgment.
Taken together, these priorities define a practical path from dataset construction to model development, validation, and deployment. They are summarized in Table 4 as an actionable research agenda for wearable AI-ECG.
6. Conclusion
Wearable AI-ECG has rapidly evolved from arrhythmia screening toward broader risk prediction and cross-system health assessment. This progression reflects a fundamental shift in ECG analysis, from detecting manifest abnormalities to uncovering latent physiological states and dynamic risk trajectories. In wearable settings, where continuous and real-world monitoring is feasible, these capabilities may substantially expand the clinical value of ECG. However, wearable AI-ECG is not simply an extension of hospital-based ECG analysis; its performance and clinical value are shaped by single- or few-lead acquisition, motion artifacts, device differences, individual variability, and long-term monitoring context.
At present, the maturity of wearable AI-ECG remains uneven across tasks: arrhythmia diagnosis is relatively established, whereas arrhythmia early warning and multi-disease prediction are promising but still limited by data scarcity, weak standardization, and incomplete clinical validation. Future progress will require advances not only in algorithms, but also in data, interpretability, deployment, and integration into clinical workflows. In particular, standardized wearable ECG datasets, artifact-aware modeling, cross-device and cross-population validation, prospective real-world evaluation, multimodal fusion, and clinically interpretable outputs will be essential for translation. If these barriers can be overcome, wearable AI-ECG may become a key platform for continuous, proactive, and personalized cardiovascular and systemic health management.
Acknowledgements
This manuscript was edited for language clarity using Grammarly. Qwen-Image (version 2.0) was used to generate the sub-figures of Figure 1 and Figure 7 illustrating the background of AI-ECG applications in cross-system diseases. The authors take full responsibility for the integrity, originality, and accuracy of the work.
Authors contribution
Li Z: Conceptualization, writing-original draft.
Tian Y, Jin Y: Writing-review & editing.
Liu C: Supervision, writing review & editing.
Conflicts of interest
Zhiyuan Li is a Youth Editorial Board of BME Horizon. The other authors declare no conflicts of interest.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
Not applicable.
Funding
This paper was partly supported by the National Natural Science Foundation of China (Grant No. 62406190), National Postdoctoral Program for Innovative Talents (Grant No. BX20230215), China Postdoctoral Science Foundation (Grant No. 2023M732219), Shanghai Municipal Science and Technology Major Project (Grant No. 2021SHZDZX0102).
Copyright
© The Author(s) 2026.
References
-
1. Chong B, Jayabaskaran J, Jauhari SM, Chan SP, Goh R, Kueh MT, et al. Global burden of cardiovascular diseases: Projections from 2025 to 2050. Eur J Prev Cardiol. 2025;32(11):1001-1015.[DOI]
-
2. Murray CJL. The global burden of disease study at 30 years. Nat Med. 2022;28(10):2019-2026.[DOI]
-
3. Taylor GJ. 150 practice ECGs: Interpretation and review. 3rd ed. New York: John Wiley & Sons; 2006.
-
4. Anliker U, Ward JA, Lukowicz P, Troster G, Dolveck F, Baer M, et al. AMON: A wearable multiparameter medical monitoring and alert system. IEEE Trans Inform Technol Biomed. 2004;8(4):415-427.[DOI]
-
5. Li D, Cui TR, Liu JH, Shao WC, Liu X, Chen ZK, et al. Motion-unrestricted dynamic electrocardiogram system utilizing imperceptible electronics. Nat Commun. 2025;16:3259.[DOI]
-
6. Attia ZI, Harmon DM, Dugan J, Manka L, Lopez-Jimenez F, Lerman A, et al. Prospective evaluation of smartwatch-enabled detection of left ventricular dysfunction. Nat Med. 2022;28(12):2497-2503.[DOI]
-
7. Siontis KC, Noseworthy PA, Attia ZI, Friedman PA. Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat Rev Cardiol. 2021;18(7):465-478.[DOI]
-
8. Zhang D, Li J, Geng S, Wang Y, Chen S, Fan S, et al. ECGomics: An open platform for AI-ECG digital biomarker discovery. arXiv:2601.15326 [Preprint]. 2026.[DOI]
-
9. Elgendi M, Elkhalifa A, Alhashmi N, Aldahmani A, Aljneibi N, Alamro D, et al. Wearable ECG and PPG for anxiety detection: A translational digital medicine perspective. npj Digit Med. 2026.[DOI]
-
10. Baraeinejad B, Shayan MF, Vazifeh AR, Rashidi D, Hamedani MS, Tavolinejad H, et al. Design and implementation of an ultralow-power ECG patch and smart cloud-based platform. IEEE Trans Instrum Meas. 2022;71:1-11.[DOI]
-
11. Davarmanesh P, Jabbour G, Lin Q, Tenison I, Stultz C, Alam R. Detection of acute myocardial infarction and ischemia from lead-I ECG using deep learning. Circulation. 2024;150(Suppl_1):A4125281.[DOI]
-
12. Han C, Song Y, Lim HS, Tae Y, Jang JH, Lee BT, et al. Automated detection of acute myocardial infarction using asynchronous electrocardiogram signals-preview of implementing artificial intelligence with multichannel electrocardiographs obtained from smartwatches: Retrospective study. J Med Internet Res. 2021;23(9):e31129.
-
13. Guo Y, Wang H, Zhang H, Liu T, Li L, Liu L, et al. Photoplethysmography-based machine learning approaches for atrial fibrillation prediction. JACC Asia. 2021;1(3):399-408.[DOI]
-
14. Ozkan H, Ozhan O, Karadana Y, Gulcu M, Macit S, Husain F. A portable wearable tele-ECG monitoring system. IEEE Trans Instrum Meas. 2020;69(1):173-182.[DOI]
-
16. Hannun AY, Rajpurkar P, Haghpanahi M, Tison GH, Bourn C, Turakhia MP, et al. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat Med. 2019;25(1):65-69.[DOI]
-
17. Jin Y, Li Z, Wang M, Liu J, Tian Y, Liu Y, et al. Cardiologist-level interpretable knowledge-fused deep neural network for automatic arrhythmia diagnosis. Commun Med. 2024;4:31.[DOI]
-
18. Liu G, Han X, Tian L, Zhou W, Liu H. ECG quality assessment based on hand-crafted statistics and deep-learned S-transform spectrogram features. Comput Meth Programs Biomed. 2021;208:106269.[DOI]
-
19. Romero FP, Piñol DC, Vázquez-Seisdedos CR. DeepFilter: An ECG baseline wander removal filter using deep learning techniques. Biomed Signal Process Control. 2021;70:102992.[DOI]
-
21. Le KH, Pham HH, Nguyen TBT, Nguyen TA, Thanh TN, Do CD. LightX3ECG: A lightweight and eXplainable deep learning system for 3-lead electrocardiogram classification. Biomed Signal Process Control. 2023;85:104963.[DOI]
-
22. Wei X, Li Z, Tian Y, Wang M, Jin Y, Ding W, et al. Spatial-temporal hierarchical decoupled masked autoencoder: A self-supervised learning framework for electrocardiogram. Expert Syst Appl. 2026;298:129603.[DOI]
-
23. Lai J, Tan H, Wang J, Ji L, Guo J, Han B, et al. Practical intelligent diagnostic algorithm for wearable 12-lead ECG via self-supervised learning on large-scale dataset. Nat Commun. 2023;14:3741.[DOI]
-
24. Smital L, Haider CR, Vitek M, Leinveber P, Jurak P, Nemcova A, et al. Real-time quality assessment of long-term ECG signals recorded by wearables in free-living conditions. IEEE Trans Biomed Eng. 2020;67(10):2721-2734.[DOI]
-
25. Zhang J, Lin JL, Li XL, Wang WQ. ECG signals denoising method based on improved wavelet threshold algorithm. In: 2016 IEEE Advanced Information Management, Communicates, Electronic and Automation Control Conference (IMCEC); 2016 Oct 3-5; Xi’an, China. Piscataway: IEEE; 2016. p. 1779-1784.[DOI]
-
26. Wang N, Feng P, Ge Z, Zhou Y, Zhou B, Wang Z. Adversarial spatiotemporal contrastive learning for electrocardiogram signals. IEEE Trans Neural Netw Learn Syst. 2024;35(10):13845-13859.[DOI]
-
27. Han H, Lian C, Zeng Z, Xu B, Zang J, Xue C. Multimodal multi-instance learning for long-term ECG classification. Knowl Based Syst. 2023;270:110555.[DOI]
-
28. Zhang P, Chen Y, Lin F, Wu S, Yang X, Li Q. Semi-supervised learning for automatic atrial fibrillation detection in 24-hour holter monitoring. IEEE J Biomed Heal Inform. 2022;26(8):3791-3801.[DOI]
-
29. Ismail H, Serhani MA, Hussein NM, Elhadef M. RL-ECGNet: Resource-aware multi-class detection of arrhythmia through reinforcement learning. Appl Intell. 2023;53(24):30927-30939.[DOI]
-
30. Tian Y, Li Z, Jin Y, Wang M, Wei X, Zhao L, et al. Foundation model of ECG diagnosis: Diagnostics and explanations of any form and rhythm on ECG. Cell Rep Med. 2024;5(12):101875.[DOI]
-
32. Wagner P, Strodthoff N, Bousseljot RD, Kreiseler D, Lunze FI, Samek W, et al. PTB-XL, a large publicly available electrocardiography dataset. Sci Data. 2020;7:154.[DOI]
-
33. Martis RJ, Acharya UR, Min LC. ECG beat classification using PCA, LDA, ICA and Discrete Wavelet Transform. Biomed Signal Process Control. 2013;8(5):437-448.[DOI]
-
34. Wei X, Li Z, Tian Y, Wang M, Liu J, Jin Y, et al. Differentiated knowledge distillation: Patient-specific single-sample personalization for electrocardiogram diagnostic models. Eng Appl Artif Intell. 2024;136:108880.[DOI]
-
36. Satija U, Ramkumar B, Manikandan MS. A review of signal processing techniques for electrocardiogram signal quality assessment. IEEE Rev Biomed Eng. 2018;11:36-52.[DOI]
-
37. Tripathi PM, Kumar A, Komaragiri R, Kumar M. A review on computational methods for denoising and detecting ECG signals to detect cardiovascular diseases. Arch Comput Meth Eng. 2022;29(3):1875-1914.[DOI]
-
38. Hu L, Cai W, Chen Z, Wang M. A lightweight U-Net model for denoising and noise localization of ECG signals. Biomed Signal Process Control. 2024;88:105504.[DOI]
-
39. Jin Y, Qin C, Liu J, Liu Y, Li Z, Liu C. A novel deep wavelet convolutional neural network for actual ECG signal denoising. Biomed Signal Process Control. 2024;87:105480.[DOI]
-
40. Wang X, Chen B, Zeng M, Wang Y, Liu H, Liu R, et al. An ECG signal denoising method using conditional generative adversarial net. IEEE J Biomed Health Inform. 2022;26(7):2929-2940.[DOI]
-
41. Li H, Ditzler G, Roveda J, Li A. DeScoD-ECG: Deep score-based diffusion model for ECG baseline wander and noise removal. IEEE J Biomed Heal Inform. 2024;28(9):5081-5091.[DOI]
-
42. Sun Z, Wang C, Tian E, Yin Z. ECG signal classification via combining hand-engineered features with deep neural network features. Multimed Tools Appl. 2022;81(10):13467-13488.[DOI]
-
43. Elhaj FA, Salim N, Harris AR, Swee TT, Ahmed T. Arrhythmia recognition and classification using combined linear and nonlinear features of ECG signals. Comput Meth Programs Biomed. 2016;127:52-63.[DOI]
-
44. Li Q, Rajagopalan C, Clifford GD. Ventricular fibrillation and tachycardia classification using a machine learning approach. IEEE Trans Biomed Eng. 2014;61(6):1607-1613.[DOI]
-
45. Melgani F, Bazi Y. Classification of electrocardiogram signals with support vector machines and particle swarm optimization. IEEE Trans Inf Technol Biomed. 2008;12(5):667-677.[DOI]
-
46. Arpitha Y, Madhumathi GL, Balaji N. Spectrogram analysis of ECG signal and classification efficiency using MFCC feature extraction technique. J Ambient Intell Humaniz Comput. 2022;13(2):757-767.[DOI]
-
47. Yao Q, Wang R, Fan X, Liu J, Li Y. Multi-class Arrhythmia detection from 12-lead varied-length ECG using Attention-based Time-Incremental Convolutional Neural Network. Inf Fusion. 2020;53:174-182.[DOI]
-
48. Jin Y, Li Z, Tian Y, Wei X, Liu C. A self-supervised framework for computer-aided arrhythmia diagnosis. Appl Soft Comput. 2024;164:112024.[DOI]
-
49. Nolin-Lapalme A, Mila—Québec AI Institute Montreal Quebec HS H, Sowa A, et al. Foundation models for electrocardiogram interpretation: Clinical implications. Eur Heart J. 2026;47(18):2174-2186.[DOI]
-
50. Liu R, Bai Y, Yue X, Zhang P. Teaching multimodal LLMs to comprehend 12-lead electrocardiographic images. npj Digit Med. 2026;9:349.[DOI]
-
51. Liu N, Sun M, Wang L, Zhou W, Dang H, Zhou X. A support vector machine approach for AF classification from a short single-lead ECG recording. Physiol Meas. 2018;39(6):064004.[DOI]
-
52. Yang S, Lian C, Zeng Z, Xu B, Zang J, Zhang Z. A multi-view multi-scale neural network for multi-label ECG classification. IEEE Trans Emerg Top Comput Intell. 2023;7(3):648-660.[DOI]
-
53. Jin Y, Li Z, Tian Y, Wei X, Liu C. A novel interpretable multilevel wavelet decomposition deep network for actual heartbeat classification. Sci China Technol Sci. 2024;67(6):1842-1854.[DOI]
-
54. Perez MV, Mahaffey KW, Hedlin H, Rumsfeld JS, Garcia A, Ferris T, et al. Large-scale assessment of a smartwatch to identify atrial fibrillation. N Engl J Med. 2019;381(20):1909-1917.[DOI]
-
55. Li Z, Jin Y, Tian Y, Liu J, Wang M, Wei X, et al. M-XAF: Medical explainable diagnosis system of atrial fibrillation based on medical knowledge and semantic representation fusion. Eng Appl Artif Intell. 2024;136:108890.[DOI]
-
57. Ribeiro AH, Ribeiro MH, Paixão GMM, Oliveira DM, Gomes PR, Canazart JA, et al. Automatic diagnosis of the 12-lead ECG using a deep neural network. Nat Commun. 2020;11:1760.[DOI]
-
58. Sangha V, Mortazavi BJ, Haimovich AD, Ribeiro AH, Brandt CA, Jacoby DL, et al. Automated multilabel diagnosis on electrocardiographic images and signals. Nat Commun. 2022;13:1583.[DOI]
-
59. Ayano YM, Schwenker F, Dufera BD, Debelee TG. Interpretable machine learning techniques in ECG-based heart disease classification: A systematic review. Diagnostics. 2023;13(1):111.[DOI]
-
60. Holzinger A, Biemann C, Pattichis CS, Kell DB. What do we need to build explainable AI systems for the medical domain? arXiv:1712.09923 [Preprint]. 2017.[DOI]
-
62. Attia ZI, Noseworthy PA, Lopez-Jimenez F, Asirvatham SJ, Deshmukh AJ, Gersh BJ, et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet. 2019;394(10201):861-867.[DOI]
-
63. Parsi A, Glavin M, Jones E, Byrne D. Prediction of paroxysmal atrial fibrillation using new heart rate variability features. Comput Biol Med. 2021;133:104367.[DOI]
-
64. Boon KH, Khalil-Hani M, Malarvili MB, Sia CW. Paroxysmal atrial fibrillation prediction method with shorter HRV sequences. Comput Meth Programs Biomed. 2016;134:187-196.[DOI]
-
66. Gilon C, Grégoire JM, Hellinckx J, Carlier S, Bersini H. Reproducibility of machine learning models for paroxysmal atrial fibrillation onset prediction. In: 2022 Computing in Cardiology (CinC); 2022 Sep 4-7; Tampere, Finland. Piscataway: IEEE; 2022. p. 1-4.[DOI]
-
68. Karimulla S, Patra D. A pioneering approach for early prediction of sudden cardiac death via morphological ECG features measurement and ensemble growing techniques. Comput Electr Eng. 2024;120:109740.[DOI]
-
69. Loria-Romero M, Peregrina-Barreto H, Rangel-Magdaleno J, Rico-Aniles HD. Ventricular fibrillation characterization for sudden cardiac death risk prediction based on wavelet analysis. In: 2022 IEEE International Symposium on Medical Measurements and Applications (MeMeA); 2022 Jun 22-24; Messina, Italy. Piscataway: IEEE; 2022. p. 1-6.[DOI]
-
70. Kaspal R, Alsadoon A, Prasad PWC, Al-Saiyd NA, Nguyen TQV, Pham DTH. A novel approach for early prediction of sudden cardiac death (SCD) using hybrid deep learning. Multimed Tools Appl. 2021;80(5):8063-8090.[DOI]
-
71. Yang J, Sun Z, Zhu W, Xiong P, Du H, Liu X. Intelligent prediction of sudden cardiac death based on multi-domain feature fusion of heart rate variability signals. EURASIP J Adv Signal Process. 2023;2023(1):32.[DOI]
-
72. Huynh PK, Setty A, Phan H, Le TQ. Probabilistic domain-knowledge modeling of disorder pathogenesis for dynamics forecasting of acute onset. Artif Intell Med. 2021;115:102056.[DOI]
-
73. Li Z, Derksen H, Gryak J, Ghanbari H, Gunaratne P, Najarian K. A novel atrial fibrillation prediction algorithm applicable to recordings from portable devices. Annu Int Conf IEEE Eng Med Biol Soc. 2018;2018:4034-4067.[DOI]
-
74. Grégoire JM, Gilon C, Carlier S, Bersini H. Role of the autonomic nervous system and premature atrial contractions in short-term paroxysmal atrial fibrillation forecasting: Insights from machine learning models. Arch Cardiovasc Dis. 2022;115(6-7):377-387.[DOI]
-
75. Fujita H, Acharya UR, Sudarshan VK, Ghista DN, Sree SV, Eugene LWJ, et al. Sudden cardiac death (SCD) prediction based on nonlinear heart rate variability features and SCD index. Appl Soft Comput. 2016;43:510-519.[DOI]
-
76. Khazaei M, Raeisi K, Goshvarpour A, Ahmadzadeh M. Early detection of sudden cardiac death using nonlinear analysis of heart rate variability. Biocybern Biomed Eng. 2018;38(4):931-940.[DOI]
-
77. Shi M, He H, Geng W, Wu R, Zhan C, Jin Y, et al. Early detection of sudden cardiac death by using ensemble empirical mode decomposition-based entropy and classical linear features from heart rate variability signals. Front Physiol. 2020;11:118.[DOI]
-
78. Zhang Y, Cha X, Cui B, Lai D. Early recognition of sudden cardiac death combined with deep transfer learning and superficial ECG features. In: 2023 IEEE 4th International Conference on Pattern Recognition and Machine Learning (PRML); 2023 Aug 4-6; Urumqi, China. Piscataway: IEEE; 2023. p. 294-298.[DOI]
-
79. Xie CX, Wang LH, Yu YT, Ding LJ, Yang T, Kuo IC, et al. Clinical sudden cardiac death risk prediction: A grid search support vector machine multimodel base on ventricular fibrillation visualization features. Comput Electr Eng. 2025;123:110022.[DOI]
-
80. Chen H, Das S, Morgan JM, Maharatna K. Prediction and classification of ventricular arrhythmia based on phase-space reconstruction and fuzzy c-means clustering. Comput Biol Med. 2022;142:105180.[DOI]
-
81. Li Z, Tian Y, Jin Y, Wei X, Wang M, Liu J, et al. An early warning method for arrhythmias in long-term ECGs based on self-supervised learning and LSTM. Knowl Based Syst. 2025;327:114137.[DOI]
-
82. Fiorina L, Carbonati T, Narayanan K, Li J, Henry C, Singh JP, et al. Near-term prediction of sustained ventricular arrhythmias applying artificial intelligence to single-lead ambulatory electrocardiogram. Eur Heart J. 2025;46(21):1998-2008.[DOI]
-
83. Gavidia M, Zhu H, Montanari AN, Fuentes J, Cheng C, Dubner S, et al. Early warning of atrial fibrillation using deep learning. Patterns. 2024;5(6):100970.[DOI]
-
84. Dhingra LS, Aminorroaya A, Pedroso AF, Khunte A, Sangha V, McIntyre D, et al. Artificial intelligence–enabled prediction of heart failure risk from single-lead electrocardiograms. JAMA Cardiol. 2025;10(6):574.[DOI]
-
85. Sangha V, Dhingra LS, Aminorroaya A, Croon PM, Sikand NV, Sen S, et al. Identification of hypertrophic cardiomyopathy on electrocardiographic images with deep learning. Nat Cardiovasc Res. 2025;4(8):991-1000.[DOI]
-
86. Bouzid Z, Sejdic E, Martin-Gill C, Pa UP, Faramand Z, Frisch S, et al. Electrocardiogram-based machine learning for risk stratification of patients with suspected acute coronary syndrome. Eur Heart J. 2025;46(10):943-954.[DOI]
-
87. Bock C, Walter JE, Rieck B, Strebel I, Rumora K, Schaefer I, et al. Enhancing the diagnosis of functionally relevant coronary artery disease with machine learning. Nat Commun. 2024;15:5034.[DOI]
-
88. Poterucha TJ, Jing L, Ricart RP, Adjei-Mosi M, Finer J, Hartzel D, et al. Detecting structural heart disease from electrocardiograms using AI. Nature. 2025;644(8075):221-230.[DOI]
-
90. Lima EM, Ribeiro AH, Paixão GMM, Ribeiro MH, Pinto-Filho MM, Gomes PR, et al. Deep neural network-estimated electrocardiographic age as a mortality predictor. Nat Commun. 2021;12:5117.[DOI]
-
91. Samek W, Montavon G, Lapuschkin S, Anders CJ, Muller KR. Explaining deep neural networks and beyond: A review of methods and applications. Proc IEEE. 2021;109(3):247-278.[DOI]
Copyright
© The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Publisher’s Note
Science Exploration remains a neutral stance on jurisdictional claims in published
maps
and institutional affiliations. The views expressed in this article are solely those
of
the author(s) and do not reflect the opinions of the Editors or the publisher.
Share And Cite



Science Exploration Style
Li Z, Tian Y, Jin Y, Liu C. AI-ECG for wearable monitoring: From arrhythmia diagnosis to early warning and multi-disease prediction. BME Horiz. 2026;4:202619. https://doi.org/10.70401/bmeh.2026.0029
Tips
Copy completed.
Submit a Manuscript
Author Instructions
Cite this Article
Article Metrics
0
View
0
Download
Cited
Article Updates

- Abstract
- Keywords
- 1. Introduction
- 2. Overview of AI-ECG for Wearable Monitoring
- 3. AI-ECG for Arrhythmia Diagnosis
- 4. Frontier Extensions of AI-ECG in Wearable Monitoring
- 5. Challenges and Future Perspectives
- 6. Conclusion
- Acknowledgements
- Authors contribution
- Conflicts of interest
- Ethical approval
- Consent to participate
- Consent for publication
- Availability of data and materials
- Funding
- References
- Copyright
Science Exploration Style
Li Z, Tian Y, Jin Y, Liu C. AI-ECG for wearable monitoring: From arrhythmia diagnosis to early warning and multi-disease prediction. BME Horiz. 2026;4:202619. https://doi.org/10.70401/bmeh.2026.0029
copy
Share Link
copy