Improvement of a BCI-enabled Boccia ramp through a patient engagement strategy
Daniel Comaduran Marquez
1,*

,
Daniella Bourque
2
,
Dejana Nikitovic
1
,
Alicia Hilderley
1
,
Eli Kinney-Lang
2
,
Iulian Ciobanu
3
,
Alison Levine
3
,
Adam Kirton
1,4
*Correspondence to:
Daniel Comaduran Marquez, Cumming School of Medicine, University of Calgary, Calgary, Alberta, T2N 1N4, Canada.
E-mail: dcomadur@ucalgary.ca
Empath Comput. 2026;2:202531. 10.70401/ec.2026.0020
Received: October 25, 2025Accepted: March 25, 2026Published: March 27, 2026
This article belongs to the Special lssue Co-creation for accessible computing through advances in emerging technologies
This manuscript is made available in its unedited form to allow early access to the
reported findings. Further editing will be completed before final publication. As such,
the content may include errors, and standard legal disclaimers are applicable.
Abstract
Aims: The right to play is a basic human right. However, sport participation is often limited for children with complex motor disabilities such as quadriplegic cerebral palsy. Brain-computer interface systems (BCIs) translate a user’s brain waves into instructions that can be used to control external devices. We have developed a BCI-enabled Boccia system that allows children who cannot move on their own to play independently. Boccia is a Paralympic sport that offers inclusion for individuals with limited mobility, it does not fully accommodate those with severe motor disabilities and communication difficulties. The purpose of this study was to partner with persons with lived experience (PWLE) to improve the Boccia system with the expertise of patients and Boccia Paralympic athletes.
Methods: Following the Strategy for Patient Oriented Research (SPOR) framework, we engaged seven PWLE to participate in two virtual sessions and one in-person session to improve the BCI-Boccia system. After the first virtual session, the engineering team translated the feedback and comments from the PWLE into a list of tasks to develop the new features. The software development approach used an Agile development strategy, after which the second session consisted of a demonstration to gather additional feedback for refinement. After the hardware was developed, two PWLE attended in-person sessions to use the system and provide additional feedback. Engagement was evaluated using the Public and Patient Engagement Evaluation Tool (PPEET).
Results: Comments from the first virtual meeting focused on improving the software controller of the ramp, as well as the mechanical stability of the ramp. A new software controller was designed. The coarse-movement controller is used for initial control to give the player a broad range of selection options. To refine the precision of the shot, a fine-movement controller is provided. From these two visual control schemes, both ball elevation and ramp rotation can be chosen with a single selection. Similarly, a new base for the Boccia ramp was developed to allow for improved stability and faster assembly and disassembly procedures. The results of the PPEET confirmed that the PWLE perceived that their suggestions were taken into account and that the necessary resources were provided for their participation.
Conclusion: We demonstrate that a patient engagement strategy can inform and facilitate improvements to a BCI-enabled Boccia system. The resulting system supports the play of both recreational and competitive users by having a simplified controller and improved hardware. Involving diverse PWLE throughout the design cycle may improve accessibility and user adoption in disability sports. Inclusive participation likely helps ensure that improvement efforts directly address the needs of end users.
Keywords
Brain-computer interface, inclusive sports, Boccia, patient engagement, persons with lived experience
1. Introduction
The opportunity for children living with disability to engage in play is formally recognized as a basic human right in the Conventions of the Rights of the Child[1], and Persons with Disabilities[2]. In addition to the physical benefits of sports, there is substantial evidence that team sports offer many psychological and social health benefits for children and adolescents[3]. However, sport participation, even through adapted sports, can remain inaccessible for children with the most complex motor needs, such as those living with quadriplegic cerebral palsy. Such youth are often highly cognitively capable but are physically “locked-in”, completely unable to move or speak, resulting in isolation and exclusion from activities and full participation in life[4].
The main barriers for children with complex motor needs to access sports may include personal, social, environmental, policy and program related factors. Personal barriers may relate to the physical limitations of the disability itself including difficulties with even simple movements or communication. Social barriers might arise from negative attitudes or lack of understanding from peers, coaches, and parents (e.g., social exclusion by teammates, or lack of encouragement by parents)[5]. Environmental barriers include a lack of accessible facilities, properly adapted sports equipment, or specially trained staff[6]. Lastly, policy and program barriers may arise from the absence of inclusive sports policies, insufficient funding, and limited coordination between disability advocacy and sport organizations[6]. Such restricted access to sports activities for children and youth deprive them of important life opportunities[7], highlighting the need for innovation.
Brain-computer interface (BCI) technology offers a potential solution to allow truly inclusive participation for people living with complex disabilities. Typical non-invasive BCI systems work by measuring electrical brain activity with electroencephalography (EEG) electrodes placed on the scalp. Through different BCI control paradigms (e.g., motor imagery, evoked-response potentials,
Critically, children have also been almost entirely excluded from the rapid growth in BCI research[11]. This is despite growing evidence that simple BCI systems can be used effectively by school-aged children with complex motor needs to perform a variety of personally meaningful tasks[12-14]. As young learners, children and youth are excellent BCI candidates, potentially receiving lifelong benefits across diverse elements of quality of life[11,15]. Recent patient engagement efforts have confirmed the great interest of children and their families in developing new BCI applications including sports[16].
True patient engagement has become a cornerstone of health research[17]. Inclusion of end-users, at all stages from ideation to
In the Paralympics, Boccia shines as a sport that offers successful accommodations for persons living with different levels of physical disability. Boccia is a precision Paralympic sport in which individuals or teams propel a ball towards a common target (i.e., jack
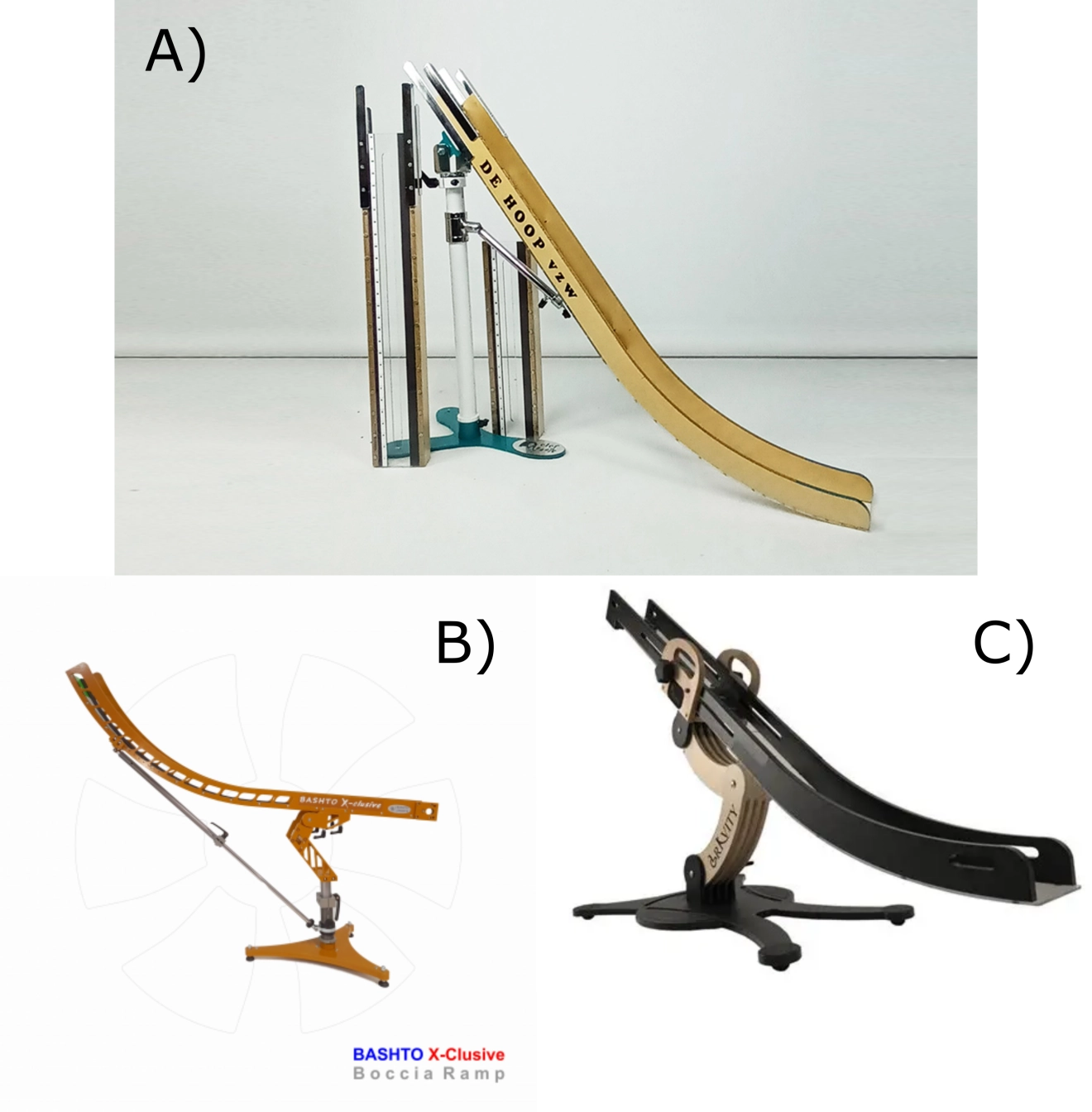
Figure 1. Examples of boccia ramps. (A) Elef Boccia Ramps; (B) Bashto Sports; (C) Gravity Boccia.
We have started to develop an early prototype of a BCI-enabled Boccia system[24]. This consists of a physical Boccia ramp with motors to control the rotation of the ramp, as well as the elevation and release mechanisms for the Boccia ball. The BCI-enabled Boccia ramp bypasses the need for a ramp operator, allowing children who cannot move or speak to play Boccia with minimal assistance using only their own thoughts. This initial prototype was created by one-time consultation between our multidisciplinary BCI clinical research team and Boccia athletes, coaches, and organizers of a local Boccia recreational league. Further development requires a formal patient engagement approach that will be essential if we are to close the persistent usability gap found in the translation of BCI technologies from research into practice[25]. Thus, the objective of this project was to apply a structured engagement of persons with lived experience (PWLE) to improve the BCI-enabled Boccia ramp.
2. Methods
2.1 Engaging persons with lived experience
We invited a total of seven PWLE to join our research team. We use the broader term PWLE as our partners include individuals who have a motor disability, are users of BCI technology, or have experience playing Boccia in recreational or professional settings. Partners included youth and families from our BCI clinical program, and Boccia Paralympians through previous collaborations with Paralympic sports committees. From the PWLE, two had previous experience using BCIs. We followed the guiding principles of the Strategy for Patient-Oriented Research (SPOR) Framework[26], namely inclusiveness, mutual respect, support, and co-build. We approached our partnership to achieve a minimum criteria score of two on the Patient-Oriented Research Level of Engagement Tool (PORLET 2.0)[27]. A level two in PORLET corresponds to obtaining patients’ feedback on the research project and decisions. All partners were remunerated for their time following SPOR guidelines[28]. The partner hourly rate was Canadian dollar (CAD) delivered through gift cards to a maximum of CAD. Out-of-pocket expenses were reimbursed, such as parking or transportation fees and childcare.
We used the Public and Patient Engagement Evaluation Tool (PPEET) to evaluate the engagement. The PPEET includes questions designed to systematically assess the quality and impact of engagement activities from the participants’ perspective[29]. The reporting of engagement followed the short form of the GRIPP2 reporting recommendations for patient and public involvement in research[30]. Partners were informed that completing the survey would imply their consent for the collected data to be made available for the purpose of the study. Study methods were approved by the Conjoint Health Research Ethics Board at the University of Calgary (Ethics ID: REB22-1706).
2.2 Design and development
The design and development cycle is described as follows and summarized in Figure 2. Two virtual sessions were scheduled about six months apart. Both sessions were completed online using Zoom (Zoom Communications, San Jose, USA) to accommodate for PWLEs located in different cities. The first session consisted of a one-hour long session in which the PWLE and engineering team first introduced themselves. The engineers then provided a concise overview of Boccia as a Paralympic sport, the current state of the
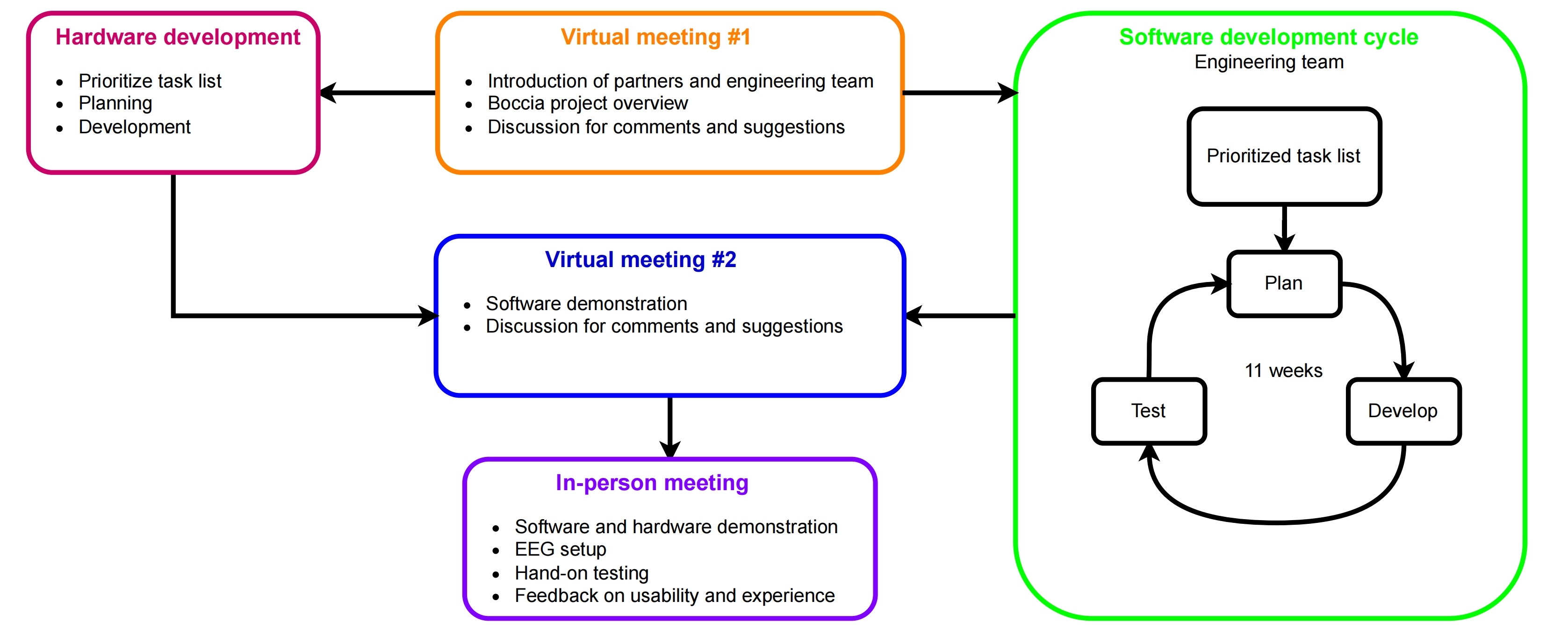
Figure 2. Development design diagram. The hardware development cycle consisted of a single development iteration. The software development cycle consisted of weekly sessions of software planning, development, and testing.
The current BCI-enabled Boccia system is described in detail elsewhere[24]. In short, the BCI-enabled Boccia system uses a front-end written in Unity (Unity Software Inc., San Francisco, USA) and the BCI-Essentials-Unity software package[31]. The signal processing backend is the BCI-Essentials-Python package implemented in Python 3.10[32]. The front and backend use streaming markers to communicate through the Lab Streaming Layer software network ecosystem[33].
Following the first virtual session, the PPEET was shared electronically via Qualtrics (Qualtrics International, Seattle, USA) to evaluate the perception of engagement quality post-development. To address the comments and suggestions from the first session, the engineering team took an approach based on Agile methodology[34]. Agile is a project management and software development approach that emphasizes breaking projects into smaller, manageable parts called iterations or sprints. It focuses on collaboration, flexibility, continuous improvement, and delivering working products frequently to satisfy customer needs.
The engineering team used the summary of the first virtual session, including the feedback and comments from the PWLE, to create a prioritized task list to lead the hardware and software development. The engineering team proceeded to work on the development of the features with weekly sessions to present progress updates among themselves, and discuss implementation strategies in case any roadblocks were found during development. Regarding hardware improvements, all parts were first modeled using Fusion 360 (Autodesk, San Francisco, USA), and then manufactured at the University of Calgary Engineering Makerspace. The software and hardware development cycle spanned eleven and twenty weeks, respectively.
The second session consisted of a detailed demonstration of advancements completed in the first Agile development cycle. Additional feedback, critiques, and suggestions were sought from the PWLE. This second virtual session was also recorded and documented through Zoom to ensure that the PWLE perspectives were effectively captured. Following this second session, the PPEET was shared electronically again with the PWLE. There was no additional development done on the software or hardware following the second session. During the second session, local PWLE were also invited to attend a one-hour in-person testing session for hands-on feedback.
2.3 In-person session
Two partners attended the in-person session. During the in-person session, the PWLE were fitted with a 7 channel DSI-flex EEG system (Wearable sensing, San Diego, USA) for testing the prototype. The electrodes were placed over the central and parietal areas, roughly covering C5 to C6, and P5 to P6 in the 10-10 configuration. Data were sampled at 300 Hz and band-pass filtered between 0.1 and 10 Hz with a 4th order digital Butterworth filter. This headset was chosen over traditional gel-based EEG systems to simplify the setup procedure and focus the session time on the usability testing. The BCI system used a P300 paradigm that was previously validated using the original software[24]. The PWLE were encouraged to operate the system and test all the integrated functions to provide additional feedback on usability and experience. The system was set up in a gymnasium inside the Alberta Children’s Hospital facilities to allow the partners to mimic a game of Boccia in which they would control the ramp movements and drop the ball. The purpose of this session was to capture feedback and usability, rather than evaluate BCI use through metrics such as calibration scores and accuracy.
3. Results
3.1 Virtual session #1
The seven PWLE attended the first virtual session. Following the session, the recording was transcribed and the summarized comments and suggestions were distributed over email (Table 1). The engineering team suggested that if it would be useful to have an virtual play mode to allow for players to use at home, partners agreed that this mode could be useful to cater to both professional players who would like to practice, and recreational players who would use it for leisure.
Table 1. Key comments and future design suggestions from the first virtual session.
| Topic | Comments | Suggestions |
| Ramp stability | - Ramp must not move after positioning - Castor wheels cause movement that affect accuracy - Most athletes avoid using ramp extensions | - Use stronger castor wheels to maintain stability - Prioritize stable base design to improve shot accuracy |
| Ramp set-up time | - Athletes have 6 minutes per game to position the ramp - Avoid extensions as they increase set up time- Concern for slow setup even in recreational play | - Design setup should be quick and straightforward - Minimize adjustments/additions that increase setup time |
| Ramp movement between shots | - Ramp must be moved between turns - Moving the ramp should be fast and simple | - Ramp should be lightweight yet stable - Explore multiple wheel models for movement and stability |
| Size of ramp | - Small base allows positioning from anywhere in throwing box - Correct rail spacing to prevent ball from rolling to one side | - Keep ramp base compact for maneuverability - Ensure correct rail spacing to maintain proper ball trajectory |
| Speed of ball | - Speed depends on height at which ball is released - Pushing the ball has little effect on speed - Heavier balls are chosen for displacement shots | - Allow ball release from any point in ramp for speed - Focus on height adjustment and ball type selection |
| Ramp control selection | - Precise aim and height control are essential for accuracy - Fine adjustments are critical for shot performance | - Implement dual controls for coarse and fine movement adjustments - Controller should allow subtle positional tweaks to optimize accuracy |
| Software realism | - The current view does not resemble the position of an actual Boccia ramp from the players’ perspective - The current court does not have any of the dimensions of a real Boccia court | - The software should try to resemble the view of the Boccia ramp from the perspective of the player - The court should have real dimensions and markings as a Boccia court |
After the session, the engineering team created a hardware and a software development task list. The software development task focused on the ramp control selection. The original software prototype had a controller as described in detail elsewhere[24]. In short, the first software iteration used a two-step process to select the ramp movements: The main screen has buttons for height, rotation, and drop actions (Figure 3A). If height or rotation were selected, the secondary menu changes to “Up” and “Down”, or “Left” and “Right”, accordingly (Figure 3B). The secondary screen includes a “Back” button to navigate to the main screen. Each selection in the secondary screen has a predefined step size (e.g., every “Up” selection would move the ball up by a set amount, say 3 cm). Thus, we opted for position-based mechanisms with coarse- (Figure 3C) and fine-movement (Figure 3D) controllers to control rotation and height with a single selection. To address feedback about the ramp size and ball speed, we refined the visuals to better match a real Boccia setup. For example, based on partners’ feedback, we focused on adding a secondary view with a more realistic camera perspective from the player’s position following the Virtual Session 1. Lastly, to allow players to practice at home, we developed two different play modalities: Play Boccia and Virtual Play. In the Play Boccia modality, players can connect the software to the real-world ramp to play with peers in person, whereas the Virtual Play mode allows players to practice without the need for the physical ramp.
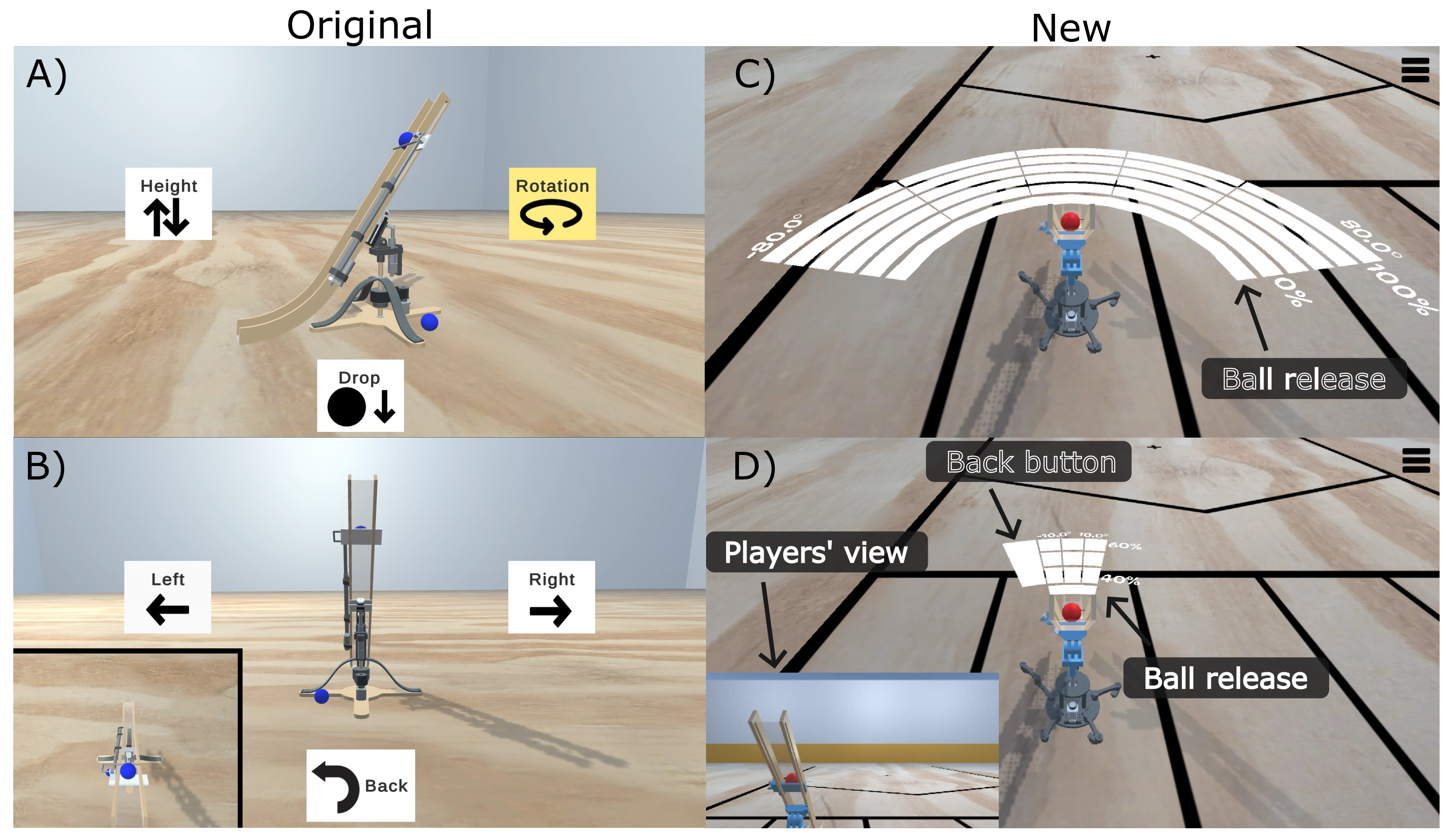
Figure 3. Screenshots of the original software interface showing the main screen (A), and the secondary screen after selecting the “rotation” option (B). Screenshots of the new software interface showing the coarse- (C) and fine-movement (D) controllers. Note the updated secondary view in (D) showing the ramp from the players’ perspective.
Hardware development focused on improving the stability of the ramp by modifying the base (Figure 4). The main suggestions from the PWLE were that the base of the ramp should be modified to improve stability as this affects shot accuracy (Table 1). Additionally, the PWLE commented that the ramp needed to be easier to move because the play time is limited (i.e., 6 min per turn) and suggested that the current castors might cause unwanted movements after a shot is completed.

Figure 4. (A) Original ramp base; (B) Modified ramp base based on the comments and suggestions from the first virtual session.
Thus, the engineering team focused on creating a new base. The new base was modeled based on a commercially available rolling floor stand (Ideas for Independent Living, Inc., Scarborough, Canada). The new base is made of aluminum and has five heavy-duty castors. The added weight from the aluminum, in addition to the heavy-duty castors, make this base much more stable than the original model. A module to host the rotation mechanism was developed to match the dimensions of the rolling floor stand. To address the comments regarding the ramp setup time and the movement between shots, this module was designed to be easily mounted and dismounted.
3.2 Virtual session #2
Four PWLE attended the second virtual session due to personal time constraints. The main takeaway points were the following:
∙ The PWLE commented on the improved realistic representation of the ramp with the addition of the court limits.
∙ The new coarse- and fine-movement controllers were well received. Partners commented that the new controller seemed to allow for faster selections compared to the original prototype.
∙ Overall hardware stability improvements and design changes were well received.
Participants identified that implementation of the Boccia rules was missing from the Virtual Play mode. Specifically, users noted that when the Jack ball goes out of bounds, the software should reposition the ball at the center of the court. Feedback also emphasized the need to preserve the position of the ramp between consecutive shots, allowing the user to continue playing from their prior configuration. Additional discussion revolved around user interface clarity, with suggestions to offer optional labels for rotation and elevation so users could tailor the display to their experience level. Supplemental modes for training and at-home practice were displayed, emphasizing their value in facilitating skill acquisition and adaptation outside competitive environments. The PWLE commented that the Virtual Play mode should resemble the real game speed to allow for a valid practice experience for the player. Accessibility features were reviewed in response to concerns about visual interface elements such as flashing buttons, with consideration given to alternative control software suited for users with photosensitivity. The ongoing challenges of balancing visual cues with control precision were discussed.
Hardware improvements were also presented. The engineering team outlined modifications to the ramp base, and a redesign of the incline mechanism. These changes were done with the setup time in mind, and allow for easier assembly, disassembly, and transport. Visual comparisons highlighted the changes made from the first prototype. The PWLE suggested that these changes substantially enhanced the system functionality and stability.
Future development directions were also discussed. These included consideration of a motorized incline controller, using alternative input devices (e.g., joysticks, sip and puff devices), and additional BCI paradigms (e.g., auditory P300, motor imagery) to expand accessibility and user control. In summary, the second virtual session facilitated a review of the technical improvements, and confirmed that most of the initial suggestions were addressed.
3.3 In-person testing session
Two PWLE attended the in-person testing. During the session, the PWLE used the system with different types of flashing stimuli (e.g., solid color flashing, gradients flashing, different types of face sprites). One of the PWLE mentioned that it would be useful to be able to use face sprites of family or friends in order to personalize the experience. Additionally, the PWLE tested different numbers of selectable objects. Both PWLE mentioned that the system was simpler to use with a smaller number of selectable objects in the coarse- and fine-movement controller. They also mentioned that the spacing between the selectable objects of the controllers should be increased as they often felt distracted by neighboring objects. Overall, the PWLE reported that the system seemed intuitive and simple to use after being assisted with the setup of the EEG cap.
3.4 PPEET Survey
The PPEET was completed anonymously by two PWLE at the first time point and by one partner at the second time point (n = 3). Partners indicated agreement or strong agreement that they had a clear understanding of the study and that the necessary information was provided. All respondents strongly agreed that they received adequate supports to fulfill their role as research partners.
Although all agreed or strongly agreed that they were able to express their views freely and felt that their perspectives were heard, responses were neutral or agree as to whether a wide range of views was shared and whether the study team represented diverse perspectives. Participants strongly agreed that the research team considered partner feedback. Additionally, partners agreed or strongly agreed that their contributions made a meaningful difference to the study and that the project achieved its stated objective.
All respondents agreed that their participation in the study team was a worthwhile use of their time and that their involvement improved their understanding of the research. Overall satisfaction with the engagement process was high. No suggestions for improvement were provided in the open-ended questions. One partner noted a strength of the research team was that “they seem to listen very carefully to our feedback and actually implement it.”
4. Discussion
An initial prototype of the BCI-enabled Boccia system was created by one-time consultation with Boccia athletes, coaches, and organizers of a local Boccia recreational league[24]. Building on this, the current work leveraged a patient partner strategy involving both PWLE and Boccia experts to refine the system through sustained feedback and iterative development. This process not only ensured that user experience guided the technical direction, but also provided insight into developing features that improved accessibility and play realism. The effectiveness of this strategy was assessed using the PPEET validated form, allowing for reflection on the quality and depth of the PWLE involvement.
The newly developed Play Boccia and Virtual Play modes enable users to play with peers using the hardware Boccia ramp, and practice at home, respectively. These two modes allow for different levels of skill to practice the sport at their own pace. Additionally, the Virtual play mode simplifies logistical challenges, as players might have to commute to the hospital facilities to access the Boccia ramp. The redesign of the controller scheme from a two-step mechanism into the coarse- and fine-movement controller stemmed directly from the PWLE feedback (Figure 3). This modification simplified the controller to make a single selection while maintaining precision and play speed. Both of these aspects are essential for competitive Boccia according to the comments from the Boccia athletes (Table 1).
The hardware improvements focused on improving the stability of the ramp, as well as the portability during play, and the time of assembly and disassembly. By optimizing the structure of the base, the new design achieves a faster setup and tear-down without compromising mechanical integrity. These refinements can benefit both competitive and recreational users. Collectively, these modifications enhance usability, making the system easier to adopt in the professional and recreational communities.
The PPEET evaluations reflected our intentional and strong engagement approach. The PWLE that completed the PPEET evaluations felt that their contributions were heard and implemented. By creating the task list directly from the partners’ comments, the engineering team implemented the suggested features that were possible with the allocated resources. This list also helped ensure the partners that our intentions were to build a space of mutual respect in which the opinions of everyone are heard, as recommended by the SPOR framework[26]. However, it is important to note that only 3 out of the 7 partners completed the PPEET evaluations (i.e., response rate). Thus, the results presented here might not reflect the perception of all the partners that engaged in the project.
The comments from the PWLE came mostly from their personal experiences (i.e., previous use of BCI technology, Boccia at a recreational or professional level, having a physical disability). Thus, the modifications made to the BCI-Boccia system from these experiences were enriched not only by trying to solve the technical challenges, but also by making sure that the solutions still cater to the target users. For example, the new controller mechanisms allow for simplified control to keep the Boccia game accessible, while also simplifying the BCI controller by reducing the number of selections to aim the ramp to the target. To illustrate, in the original software, if the player wanted to move the ramp by three steps to the left, and two steps up, they would have to do the following selections with the BCI system: “Rotation”, “Left” three times, “Back”, “Height”, and “Up” two times. This would require a total of 8 selections. The new software would only need one selection using the coarse-movement controller, or two selections if the player wanted a more refined position using the fine-movement controller. Assuming the accuracy previously reported using the P300 paradigm, and a 4.5 sec trial duration[24], the new controller mechanisms could reduce selection time from about 39 (old design) to 9 seconds (new design) in the slowest case. However, the system needs these hypothesized improvements to be further validated in real-world Boccia games to optimize the size, number, and precision of the BCI-selectable segments.
The limitations are associated with the inherent constraints of resources typical of any development project (i.e., time, personnel, and financial support). These constraints are exacerbated in research engaging PWLE[17]. Similar to other design projects, the scope of the design had to be defined early on to better focus our efforts on obtaining a minimal viable product. Additionally, the PWLE had very limited time for the design sessions, thus impacting prototype refinement. Similarly, not all PWLE could participate in all the sessions due to personal time constraints. These limitations may have influenced the breadth and depth of design options that could have been considered for the proposed system.
Furthermore, while the PWLE engagement was essential for the project, not all feedback or suggestions could be implemented in the final design. This limitation could be due to technical or logistical constraints. The engineering team tried to balance the partners’ input with the engineering feasibility of the proposed ideas. However, there are professional and personal biases that may have contributed to the selection and implementation of certain ideas over others. Additionally, the perspectives represented by the PWLE, while invaluable, might not encompass the full diversity of experiences, preferences, and functional abilities present across the general population of potential end-users. As a result, the proposed system may not fully generalize to all users who could benefit from such a BCI-enabled Boccia system.
Future steps should continue to engage PWLE to validate the changes proposed here and further refine the BCI-Boccia system. Similar projects should consider implementing a patient engagement approach to get similar benefits to the ones described here. The development of similar BCI systems should have the same end goal as ours, to improve accessibility and increased independence of the end-users.
5. Conclusion
The work presented here uses a patient engagement approach to improve the BCI-enabled Boccia ramp system prototype. By involving PWLE, we found and addressed key usability challenges in the system’s software and hardware. These improvements might better serve recreational and professional end users. However, additional validation with the system is necessary with a broader number of potential users. The transition from a two-step control scheme to the coarse- and fine-movement controller mechanism shows how patient-driven insights can lead to more intuitive and efficient BCI interfaces. The hardware redesign prioritized ramp stability and portability to further enhance the user experience.
This study highlights the importance of engaging PWLE in the design and development cycles, aligning with broader movements in healthcare that advocate co-development methods to improve accessibility and usability. Moreover, we exemplify how BCI systems can be developed inclusively to make sport applications accessible to all users, regardless of their motor impairments. Our goal was not only to make technical improvements in the BCI system but also to have increased participation from the partners to ensure that the proposed changes would suit the needs of potential end-users.
Acknowledgements
We would like to thank the PWLE that contributed their time and expertise to this project. Their contributions were essential to the improvement of our BCI-enabled Boccia system.
Authors contribution
Comaduran Marquez D: Writing-original draft, methodology, software, funding acquisition.
Bourque D: Writing-original draft, methodology, software.
Nikitovic D, Hilderley A, Ciobanu I, Levine A: Writing-review & editing.
Kinney-Lang E: Writing-review & editing, methodology, software, funding acquisition.
Kirton A: Writing-review & editing, methodology, supervision, funding acquisition.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical approval
This project was approved by the Conjoint Health Research Ethics Board at the University of Calgary (Ethics ID: REB22-1706).
Consent to participate
Informed consent was obtained accordingly from adult participants. Participants were fully informed about the study’s purpose, procedures, risks, and benefits before consenting to participate.
Consent for publication
Not applicable.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This work was funded by the University of Calgary with support from the 2022 HBI Brain Create and 2022 ACHRI Haslam postdoctoral fellowships awarded to UCID 10145267, the 2022 Robertson fund for Cerebral Palsy Research (Grant No. 10039581), and the 2023 A-MEDICO Program (Grant No. 10044158).
Copyright
©The Author(s) 2026.
References
-
1. Assembly UG. Convention on the Rights of the Child. United Nations, Treaty Series. 1989. 1577(3):1-23.
-
2. MacKay D. The United Nations Convention on the rights of persons with disabilities. Syracuse J Int’l L & Com. 2006;34(2):323-331. Available from: https://www.proquest.com/openview/6a843d4c79dcd2490df9f849afcebbee/1?pq-origsite=gscholar&cbl=36347
-
3. Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10:98.
-
5. Barfield JP. Introduction to adaptive sport and recreation. Adapt Phys Act Q. 2025;42(1):155.[DOI]
-
6. Elipe-Lorenzo P, Diez-Fernández P, Ruibal-Lista B, López-García S. Barriers faced by people with disabilities in mainstream sports: A systematic review. Front Sports Act Living. 2025;7:1520962.[DOI]
-
8. Abiri R, Borhani S, Sellers EW, Jiang Y, Zhao X. A comprehensive review of EEG-based brain–computer interface paradigms. J Neural Eng. 2019;16(1):011001.[DOI]
-
9. Wolpaw JR, Millan JdR, Ramsey NF. Brain-computer interfaces: Definitions and principles. Handb Clin Neurol. 2020;168:15-23.[DOI]
-
10. Rashid M, Sulaiman N, Abdul Majeed APP, Musa RM, Ab Nasir AF, Bari BS, et al. Current status, challenges, and possible solutions of EEG-based brain-computer interface: A comprehensive review. Front Neurorobot. 2020;14:25.[DOI]
-
12. Hammond L, Rowley D, Tuck C, Floreani ED, Wieler A, Kim VS, et al. BCI move: Exploring pediatric BCI-controlled power mobility. Front Hum Neurosci. 2025;19:1456692.[DOI]
-
13. Jadavji Z, Zhang J, Paffrath B, Zewdie E, Kirton A. Can children with perinatal stroke use a simple brain computer interface? Stroke. 2021;52(7):2363-2370.[DOI]
-
14. Zhang J, Jadavji Z, Zewdie E, Kirton A. Evaluating if children can use simple brain computer interfaces. Front Hum Neurosci. 2019;13:24.[DOI]
-
15. Kirton A, Kinney-Lang E, Norton J, Chau T. Editorial: BCIs: Research and development in children. Front Hum Neurosci. 2023;17:1201623.[DOI]
-
16. Comaduran Marquez D, Vaandering K, Babwani A, Redquest B, Nikitovic D, Kelly D, et al. BCI sports: Exploring the potential of BCI-leveraged sport participation for children with quadriplegic cerebral palsy. Disabil Rehabil. 2026;20:1-15.[DOI]
-
17. Aiyegbusi OL, McMullan C, Hughes SE, Turner GM, Subramanian A, Hotham R, et al. Considerations for patient and public involvement and engagement in health research. Nat Med. 2023;29(8):1922-1929.[DOI]
-
18. Alonso-Valerdi LM, Mercado-Garcia VR. Updating BCI paradigms: Why to design in terms of the user? In: 2021 10th International IEEE/EMBS Conference on Neural Engineering (NER); 2021 May 4-6; Italy. Piscataway: IEEE; 2021. p. 710-713.[DOI]
-
19. Dillen A, Omidi M, Díaz MA, Ghaffari F, Roelands B, Vanderborght B, et al. Evaluating the real-world usability of BCI control systems with augmented reality: A user study protocol. Front Hum Neurosci. 2024;18:1448584.[DOI]
-
20. Lightbody G, Ware M, McCullagh P, Mulvenna MD, Thomson E, Martin S, et al. A user centred approach for developing Brain-Computer Interfaces. In: Pervasive Computing Technologies for Healthcare (PervasiveHealth) 2010; 2010 Mar 22-25; Munich, Germany. Piscataway: IEEE; 2010. p. 1-8.[DOI]
-
21. Holmes BJ, Bryan S, Ho K, McGavin C. Engaging patients as partners in health research: Lessons from BC, Canada. Healthc Manage Forum. 2018;31(2):41-44.[DOI]
-
22. Carroll SL, McGillion M, Abelson J, Berkesse A, Healey JS. Engaging patient partners to identify research priorities for atrial fibrillation: Results from a patient engagement day. PEC Innov. 2025;7:100417.[DOI]
-
23. Boccia Canada. What is Boccia? [Internet]. Ottawa (ON): Boccia Canada; 2026. Available from: https://bocciacanada.ca/en/boccia/
-
24. Marquez DC, McNutt MK, Lillywhite B, Robu I, Irvine B, Zewdie E, et al. Development and validation of a BCI-enabled boccia ramp for sport participation. In: 2023 IEEE International Conference on Systems, Man, and Cybernetics (SMC); 2023 Oct 1-4; Honolulu, USA. Piscataway: IEEE; 2023. p. 1098-1103.[DOI]
-
25. Pan H, Ding P, Wang F, Li T, Zhao L, Nan W, et al. Comprehensive evaluation methods for translating BCI into practical applications: Usability, user satisfaction and usage of online BCI systems. Front Hum Neurosci. 2024;18:1429130.[DOI]
-
26. Government of Canada CIoHR. Strategy for Patient-Oriented Research. 2018 Jun.. last Modified: 2023-11-07
-
27. Saskatchewan Centre for Patient-Oriented Research. PORLET & IRLET.
-
30. Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: Tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453.[DOI]
-
31. Irvine B, Kinney-Lang E, Wehner M. BCI-essentials-unity. 2023 Mar.
-
32. Irvine B, Kinney-Lang E, GulamHusein A. BCI-essentials-python. 2023 Mar.
-
33. Kothe C, Shirazi SY, Stenner T, Medine D, Boulay C, Grivich MI, et al. The lab streaming layer for synchronized multimodalrecording. Imaging Neurosci. 2025;3:IMAG.a.136.[DOI]
-
34. Silva LB, Jimenez RC, Blomberg N, Luis Oliveira J. General guidelines for biomedical software development. F1000Research. 2017;6:273.[DOI]
Copyright
© The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Publisher’s Note
Science Exploration remains a neutral stance on jurisdictional claims in published
maps
and institutional affiliations. The views expressed in this article are solely those
of
the author(s) and do not reflect the opinions of the Editors or the publisher.
Share And Cite



Science Exploration Style
Comaduran Marquez D, Bourque D, Nikitovic D, Hilderley A, Kinney-Lang E, Ciobanu I, et al. Improvement of a BCI-enabled Boccia ramp through a patient engagement strategy. Empath Comput. 2026;2:202531. https://doi.org/10.70401/ec.2026.0020
Tips
Copy completed.
Submit a Manuscript
Author Instructions
Cite this Article
Article Metrics
0
View
0
Download
Cited
Article Updates

Science Exploration Style
Comaduran Marquez D, Bourque D, Nikitovic D, Hilderley A, Kinney-Lang E, Ciobanu I, et al. Improvement of a BCI-enabled Boccia ramp through a patient engagement strategy. Empath Comput. 2026;2:202531. https://doi.org/10.70401/ec.2026.0020
copy
Share Link
copy